Marino - Pancreas Flashcards
(73 cards)
What is the starting point for acute pancreatic pathophys?
- Pathophysiology starts with intracellular activation of enzymes: conversion of pancreatic zymogens to their active forms within the acinar cell
- Local, systemic disease results from inflammatory processes and enzyme injury
What are the (4) protective mechanisms of the pancreatic acinar cell?
- Normal physiology protective mechanisms:
1. Inactive proenzymes
2. Membrane enclosed: no proteases in the cytoplasm
3. Separate pathways (compartments):
a. Secretory: Zymogen granules
b. Degradative: lysosomes -> can digest, activate some digestive proteases, so this sorting is important
4. Trypsin INH: scavenges activated proteases - NOTE: most efficient protein-synthesizing cell in the body

What are the normal nueronal/hormonal stimuli for pancreatic acinar cell secretion?
- Stimulus secretion COUPLING mechanism
- 1o stimulus: Ach and Ca IC signaling mechanism
- CCK/secretin: hormonal
- VIP/Ach: neuronal

What are the 2 key mechs of injury in acute pancreatitis?
- Blockage of secretion: reduction in exocytosis process due to stimulation
-
Co-localization of ZG and lysosomes, leading to premature zymogen activation and auto-digestion from within the acinar cell
1. Out of zymogen granules and into the cytoplasm, digesting the cell
2. AUTO-DIGESTION occurs from within, and expands to the rest of the pancreas

How are cytokines implicated in acute pancreatitis?
- Proteases activate complement
- C3a and C5a recruit PMNs and macrophages
- Inflammatory cells release cytokines: TNF-a, IL-1, PAF, and nitric oxide (NO)
- Vascular injury and inflammatory responses
- Local initially, then spread (in extreme cases)
What are the 3 local effects of acute pancreatitis? Clinical manifestation?
- LOCAL EFFECTS:
1. Auto-digestion of pancreas
2. Pancreatic swelling (edema)
3. Fat necrosis and hemorrhage - CLINICAL CORRELATE:
1. Pain, N/V
What is this?

- Normal pancreas: low-power view of lobules
- See attached image for high-power view

What is going on here?

-
Acute pancreatitis: low-power view of fat necrosis between lobules -> dead adipocytes (no nucleus)
1. Can still see outline of the cell, but the wall becomes crinkly, and you will eventually see macros in here - Note the septate-appearing destruction of the pancreatic parenchyma (bottom left corner)
- Compare to attached normal image

What is this? What might the micro image look like?

- Gross image of fat necrosis in between pancreatic lobules in acute pancreatitis
- MICRO: fat necrosis with outlined, wrinkled appearance of the cells
1. Vessel walls dying (necrotic), so you can’t see endothelium -> hemorrhage into these spaces

What is this? Un-labeled arrows?

-
Acute pancreatitis: microvascular leak + edema
1. Fat necrosis: outlined, wrinkled appearance
2. Acute inflammation,
3. Destruction of pancreatic parenchyma, and
4. Destruction of blood vessels (can’t see endothelium) and interstitial hemorrhage - ARROWS: pancreatic parenchyma (top L), inflam infiltrate (top R), vessel w/necrotic walls (bottom R)
- Compare to attached “normal” image

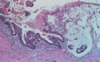
What happened here?

-
Acute pancreatitis: high-power view of:
1. Coagulative necrosis (with ghost cells),
2. Hemorrhage
3. Degenerating polys - Note residual acini in bottom right
- Normal pancreas (high-power) attached here for comparison: A = acinus, D = duct, and I = islet

What is this? Circles? Micro?

- Acute necrotizing pancreatitis (gross): red-black from hemorrhage (blue), and contains interspersed foci of yellow-white, chalky fat necrosis (green), which can usually be seen on imaging
- Vascular injury can lead to hemorrhage into the pancreatic parenchyma
- In its most severe form (hemorrhagic pancreatitis), extensive parenchymal necrosis is accompanied by dramatic hemorrhage w/in substance of the gland
- MICRO: necrosis of acinar and ductal tissues, and islets of Langerhans
- REMEMBER: islets are the COCKROACHES, so it takes a lot for them to die

What is this? Arrows? Enzymatic causes?

- Severe, acute hemorrhagic pancreatitis
- BLACK ARROW: tan and yellow areas of fat necrotis -> lipase
- GREEN ARROW: hemorrhage -> elastase causes vascular damage
What is the systemic containment response to acute pancreatitis?
- Circulating a1-antitrypsin: inactivates circulating proteases
- Circulating a-macroglobulin: binds to circulating trypsin, and facilitates monocyte clearance of macroglobulin-trypsin complexes
What are the 4 types of containment failure in sever pancreatitis? Provide the cause and clinical correlates for each.
- INFLAMMATORY: TNF-alpha, IL-6 -> fever, malaise, confusion
- VASCULAR: kallikrein activation (potent vasodilator), thrombin activation, elastase, chymotrypsin -> hypotension, DIC/hemorrhage
- RESPIRATORY: phospholipase A2 (PLA2: compromises alveolar integrity) -> hypoxemia
- METABOLIC: fat saponification -> hypocalcemia
- NOTE: these are all systemic responses; pt that is feverish, low BP, and difficulty breathing -> ICU
What are the 3 steps in acute pancreatitis pathophys?
- STEP 1: acinar cell injury
1. Insult to pancreas: ETOH, obstruction, etc.
2. IC activation of zymogens
3. Cell necrosis and auto-digestion - STEP 2: local inflammatory response
1. Cytokines/chemokines released by acinar cells, and inflammatory cells recruited
2. Inflam mediators released: TNF-alpha, IL-1
3. Pancreatic and vascular injury - STEP 3: systemic response (hours - days)
1. Circulating inflam mediators: PAF, TNF-alpha
2. Systemic inflam response syndrome (SIRS): multi-organ failure in very severe cases
What are the causes, symptoms, dx, and mgmt of acute pancreatitis?
- MAIN CAUSES: gallstones and alcohol
- MAIN SYMPTOMS: abdominal pain, N/V
- DIAGNOSIS: elevated serum amylase and lipase, inflamed pancreas on CT scan
- MGMT: IV fluids to manage hypotension, pain meds, remove stones if causative
What are the etiologies of acute pancreatitis?
- MISCELLANEOUS: autoimmune, drugs, infection, iatrogenic, hyperlipidemia, scorpion bite, trauma, shock, hypercalcemia, genetic
- SCORPION BITE: cholinergic storm, so cAMP and Ca pathways hyperstimulated
- GALLSTONES: HTN, blocking duct
- MECH: blockage of secretion, co-localization of lysosomal/zymogen synthesis, enzymatic damage

What are the diagnostic criteria for pancreatitis?
- 2 of the following 3:
1. Abdominal pain, N/V
2. Elevated serum amylase and lipase >3x upper limit of normal
a. A lot of things INC amylase and lipase, so need to be careful here -> has to be a significant elevation
3. CT imaging showing pancreatic inflammation
What are the 2 hereditary forms of pancreatitis?
- Shared feature of most forms is a defect that INC or sustains the activity of trypsin (see attached)
1. Circulating trypsin more difficult to degrade, and stays in circulation longer (His = histidine) - 40% risk of malignancy due to chronic inflam
- Implicated genes:
1. PRSS1 (7q34): serine protease 1 (trypsinogen 1); cationic trypsin, and GOF muts prevent self-inactivation (AUTO DOM, and most common)
2. CFTR (7q31): cystic fibrosis transmembrane conductance regulator; epi anion channel, & LOF muts alter fluid pressure and limit bicarb secretion, leading to inspissation of secreted fluids and duct obstruction - NOTE: muts in CFTR -> 1) DEC bicarb secretion by pancreatic ductal cells, 2) promoting protein plugs, 3) duct obstruction, and 4) devo of pancreatitis

How does pancreaticobiliary anatomy permit gallstone obstruction?
- Gallstones travel down CBD, and can get lodged right at the ampulla of vater
- This would obstruct both the CBD and pancreatic duct, leading to HTN in the pancreas

What is this? What is it used for?

- ERCP: can be used in the diagnosis of CBD stones
What 5 factors suggest gallstone etiology of pancreatitis (GAP)?
- Age >50
- Female
- Amylase >4000 IU/L
- AST >100 U/L
- Alk phos >300 IU/L
What is endoscopic papillotomy?
- Endoscopic procedure used to relieve obstruction and drain
- Tx for GAP