How does a patient take a spirometry test?
- Can be done slowly or “forced”
- Most often done as forced expiration
FVC or “Tiffeneau” manoeuvre
- Take a deep breath in
- Don’t hold your breath
- Put your lips round the outside of the tube
and blow out as hard as you can
for as long as you can
How do you interpret spirometry results?
A patient’s PFT values (except the FEV1/FVC ratio) are compared to predicted values, which are derived from a healthy population of people of the same gender and of similar age and height
What does this spirometry graph show?
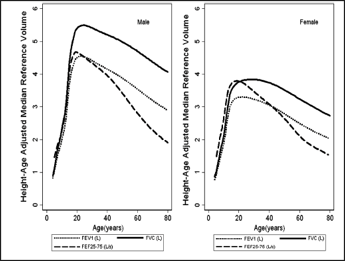
Age-related loss of lung elasticity -> decline in FVC and FEV1
What do spirometry results vary by?
Vary by gender, height, and age
What is classed as an abnormal spirometry result?
Abnormal result: any result < 80% of the predicted value
Or: any results < lower limit of normal
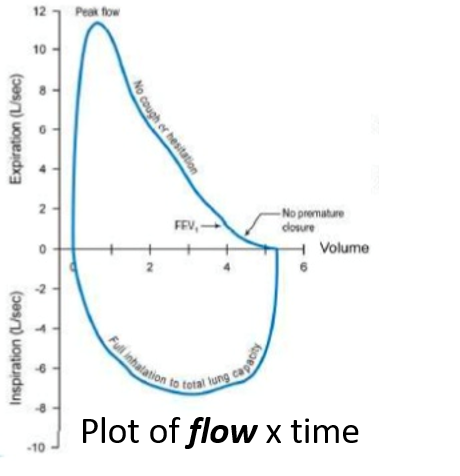
What does this show?

Normal spirometry result
What is the lower limit of normal?
The lower limit of normal (LLN) is taken to be equal to the 5th percentile of a healthy, non-smoking population
What FEVI/FVC ration shows obstruction?
FEV1/FVC ratio: should exhale > 70% of FVC in first second
If FEV1/FVC < 0.7, then obstruction is present
What does this spirometry show?

Obstruction
What does this spirometry show?

Severe obstruction
What type of graph is this?

Flow Volume loop
What does the lilac line show?

Early Airflow Obstruction
What does early airway obstruction look like on an expiratory flow-volume loop?
PEFR may be normal
Mid-Expiratory Flow Rate usually more affected
Lilac line

What does the orange line show?
What type of graph is this?

Severe Airflow Obstruction
Expiratory Flow-Volume Loop
What does the orange line show?
What type of graph is this?

Extra-Thoracic Obstruction (including tracheal stenosis, retrosternal goitre, etc)
Expiratory flow-volume loop
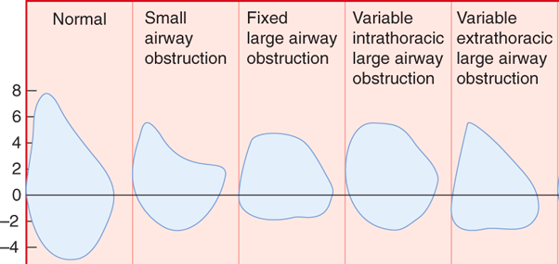
What do flow-volume loops indicate?
Flow volume loops can indicate where obstruction is located in the tracheobronchial tree
Complete the diagram on what the obstruction is in these flow-volume loops

What are the benefits of peak flow rate?
Easy to perform
Easy to maintain device
What are peak flow rates used for?
- Diagnosis – asthma, not COPD
- Monitoring day to day variation
- Picking up exacerbations
- Assessing response to treatment
The peak flow rate test is mandatory for which patients?
Asthma ptients on nebulised medicine
What does this graph show?

Peak expiratory flow
Morning dips shouldn’t be there - went with inhaled corticosteroids
consistent with diagnosis of asthma
What is the equation for flow?
Flow = (Pressure gradient) / (Raw)
Raw - airway resistance
What is the equation for airway resistance?

What could cause a decrease in the radius of an airway?
What is the consequence of this?
- Mucous or other obstruction
- Bronchoconstriction
- Compression (from a mass)
Increased resistance














-
Mechanics of breathing, pressure and work56
-
Measuring lung function46
-
Gas exchange and gas transport25
-
Respiratory failure44
-
Arterial blood gases64
-
Oxygen therapy and sleep apnoea64
-
Asthma41
-
Respiratory infections and COVID-1983
-
Imaging the thorax34
-
Chronic obstructive pulmonary disease29
-
Clinical consequences of respiratory infections42
-
Tuberculosis47
-
Interstitial lung diseases68
-
Pleural and chest wall disease45
-
Respiratory pharmacology48
-
Cough and breathlessness0
-
Occupational lung disease0
-
Imaging the normal and abnormal lung38
-
Symposium 1 - HIV and respiratory infections23
-
Symposium 2 - Lung cancer30
-
Salbutamol Practical Class6
