Miller - Sports Medicine Flashcards
(35 cards)
1
Q
Spear Tackler’s Spine
A
-
Loss of cervical lordosis, which usually helps you absorb some shock (e.g., when hit in the head)
1. Spearing can lead to load straight down on the spine, which can cause pressure fractures - Cervical stenosis: thinner region through which the spinal cord passes (inherited or acquired)
- Arthritic changes

2
Q
Stinger
A
-
Brachial plexus lesion or injury leading to stinging, burning, or electric shock sensation
1. Will come over with their arm held against their side/front - Arm numbness or weakness: will hit deltoid, biceps, rotator cuff
- Sensation of warmth
- C-5 most common: worried about cervical spine, so you will do an x-ray if this is the first one (if not, wait for the pain to relieve, then go back to play)

3
Q
C-Spine Fracture-Dislocation

A
- Mechanism: axial load most common
- Most common levels:
1. C5-6: most stress occurs here, so dislocation prone here
2. C4-5, C6-7 next

4
Q
Lower Thoracic Spine Compression Fracture
A
- Mechanism: axial load, fall
- More likely in the elderly
- Compression of vertebral body on CT; wedge-shaped formation on x-ray (see attached images)

5
Q
Stress Fracture of Pars
A
- Lumbar spine
- Symptoms: lower back pain, rare neuro symptoms
- Not a serious problem, but need to shut them down and avoid physical activity
- Can get this from doing squats
- Plain x-rays will often be normal, so you will have to do an MRI or CT to help see the extent/severity of the stress fracture
6
Q
Ruptured Lumbar Disc
A
- Symptoms: pain down leg, neuro symptoms
- Will compress nerve root, causing pain
- Young athlete may just have pain in the back of the thigh/hamstring (different presentation than older adults)

7
Q
What are the potential shoulder injuries?
A
- Rotator cuff
- Instability
- Labral tears
- AC separations
- Clavicle fractures
8
Q
What are the potential elbow injuries?
A
- OCD capitellum
- Elbow dislocation
- Biceps tendon rupture
- UCL injuries
9
Q
What are the potential wrist/hand injuries?
A
- Wrist fracture
- Scaphoid fracture
- Metacarpal fracture
- PIP dislocations
- Jersey finger
- Mallet finger
10
Q
What muscles comprise the rotator cuff?
A
- Subscapularis: subscapular fossa to lesser tubercle -> internally rotates
- Supraspinatus: supraspinous fossa to middle facet of greater tubercle -> abducts (most commonly injured)
- Infraspinatus: infraspinous fossa to posterior facet of greater tubercle -> externally rotates
- Teres minor: lateral border of the scapula to inferior facet of greater tubercle -> externally rotates

11
Q
What are the rotator cuff physical exam tests?
A
- Empty can test: supraspinatus
- External rotation: teres minor and infraspinatus
1. Stress test: infraspinatus (see attached image)
2. Lag sign: elbow passively flexed to 90° and held 5° off maximal external rotation; pt asked to maintain position while examiner releases wrist, but maintains support through the elbow -> inability to maintain the position (lag) would suggest a full-thickness tear of the rotator cuff - Pseudoparalysis

12
Q
Rotator Cuff Tear
A
- Very common: tennis players, swimmers, etc.
- Tendonitis: will often try rest, anti-inflammatory, physical therapy, and maybe a cortisone injection
- Tear: in athletes, will probably require surgery -> through small incision, stitching tendon back to the bone
13
Q
Shoulder Instability
A
- Probably 90% of the instability is going to be anterior and inferior
- May be posterior for linemen (football)
- Typically, a tear of the ligaments (glenoid)
- Risk of recurrence b/t 50 and 90%, so tendency to try and be aggressive

14
Q
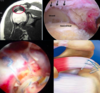
How can you reduce the shoulder (shoulder instability)?
A
- Numerous ways to get the shoulder reduced: see attached images
- Most of these involve relaxation

15
Q
Labral Tears + PE
A
- SLAP tear: superior labrum anterior to posterior
- Where biceps tendon attaches to supraglenoid tubercle via the labrum -> tearing at the attachment site
- 10 types

16
Q
SLAP/labral Tear PE
A
- O’Brien: bring arm forward, adducted across chest (w/thumb facing down), and resist downward pressure -> exacerbation of pain = (+) test
- Speed: arm straight out in front, palm up, and resist attempts to push down (biceps injury)
- Jobe: externally rotate the arm into baseball throwing position (w/pt laying down), apply anterior pressure

17
Q
AC Joint Separation
A
- First 3 classifications are the most important:
1. T1: usually a fall to the shoulder; tenderness
2. T2: complete disruption of the AC ligaments
3. T3: complete disruption of AC and choro-clavicular ligaments - Shoulder injury -> need an AP view + some kind of lateral view (axillary lateral or scapular wide)
- Posterior dislocation can fool you (humeral head and shaft will look more like a light bulb)

18
Q
What is going on in these images?

A
- AC joint separation: clinically, you will see the elevated clavicle in the upper right corner image
19
Q
Clavicle Fracture
A
- Most common is mid-shaft
- Figure 8 harness helps reduce the fracture

20
Q
OCD Capitellum (etiology and symptoms)
A
-
Etiology: unclear -> repetitive compression or interruption of blood supply (little leaguer’s elbow)
1. Articular forces during throwing: can injure lateral and/or medial side of the elbow
2. Compressive loads, or excessive axial loading (gymnasts, weight lifters)
3. Adolescent athletes 10-15 y/o; 85% males -
Symptoms: dull, poorly localized elbow pain
1. Aggravated with use, relieved with rest
2. Loose body -> catching, locking of elbow (want to prevent the development of a loose body, which will not do well long-term)

21
Q
Elbow Dislocation
A
- Describe it based on the location of the distal fragment -> posterior, anterior, lateral, medial, or divergent
- Disrupts the ligaments to the elbow
- Goal is to get it reduced -> will get stiff on you on you quick (sedation, traction/counter-traction)
- Also want to test the elbow to see just how stable it is once it has been reduced (if stable, immobilize it for about a week)

22
Q
Biceps Tendon Rupture
A
- Long head will rupture, but short belly stays intact
- Symptoms will be gone after a couple days, but they’ll get a pop-eye appearance to their biceps
- May lose about 10% of your strength of elbow flexion, but will heal (strength maintained by supportive muscles)

23
Q
Distal Biceps Tendon Rupture
A
- Ruptures on radial tuberosity
-
Functional deficits: elbow flexion, forearm rotation
1. Lose 20% of elbow flexion; 50% supination - These patients will have negative hook test (i.e., hooking finger under the biceps tendon)
- Example: someone on other end of something you are carrying drops it unexpectedly
- Laborer or young more inclined to consider surgery (but need to do this within a week or two)

24
Q
UCL Injury
A
- Ulnar collateral ligament: pain, tenderness on inside of elbow, especially when throwing
- Swelling, bruising at inner elbow (more common in acute injury; uncommon overall)
- Elbow stiffness
- Inability to throw at full speed; loss of control
- Numbness, tingling in ring and little fingers
- Clumsiness, weakness of hand grip
- 80% return to normal level of activity

25
Wrist Fracture
- Closed reduction maneuvers
- Articular involvement will require a plate
26
Scaphoid Fracture
- Often confused as a wrist sprain
- Fall on an outstretched hand
- Pain and swelling of the wrist, with soreness in the snuffbox
- If high index of suspicion (can do CT or MRI to confirm), treat these patients because you can get some bone resorption
- Take a long time to heal; up to 3 months

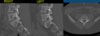
27
What do you see here?

- **Scaphoid fracture**
- X-ray on left
- CT scan on the right
28
3rd Metacarpal Fracture
- Common, esp. in football players
- Look at fingernails to make sure they look equal, side-to-side
1. Rotational abnormality will lead to fingers crossing over each other

29
4th Metacarpal Fracture
- Boxer's fracture
- Neck of the metacarpal
- Usually about 3 weeks of immobilization

30
What is this?

- _PIP joint dislocation_
- May have to recreate deformity, then push at base to reduce it
- Want to ensure patient gets full motion of the digit
- Swelling may not go all the way down
- Small fracture not a big deal, but a larger one can affect healing
31
What is this?

- _Jersey finger_: flexor tendon injury
32
What do you see here?

- _Mallet finger_: extensor tendon injury
- Can have soft tissue, or bony fracture
- Soft tissue and small bone fragments can be treated non-operatively
33
What are the common hip/pelvis injuries?
- Avulsion fractures
- Labral tears
- Quadriceps/hamstrings tears
34
What are the common knee/leg injuries?
- Meniscal injury
- Ligament injury
- Patellar instability
- Quadriceps/patellar tendon ruptures
- OCD/chondral injuries
35
What are the common foot/ankle injuries?
- Sprains
- 5th metatarsal fractures
- Lisfranc injuries
- Turf toe
- Achilles tendon rupture
