Neuro 1 Flashcards
(123 cards)
Components of neurological examination
- Assessment of awareness/level of consciousness
- Posturing
- Mental Status
- Speech Assessment
- Cranial Nerve Examination
- Cerebellar/Coordination Testing
- Gait Examination
- Motor and Strength Examination
- Reflex Testing
- Sensory Examination
Components of the Mental Status Exam (MSE)
- General appearance, behavior, and attitude
- Level of consciousness and orientation
- Speech and language
- Mood and affect
- Thought process, Content, and Perceptions
- Memory and cognition
- Judgment and insight
What level of consciousness?
- Patient is able to open eyes, look at you, and responds fully and appropriately
Alert
What level of consciousness?
- Patient is drowsy, but can open eyes, look at examiner, and respond. Falls back to sleep easily.
Lethargic
What level of consciousness?
- Patient opens eyes and looks at you, offers confused responses, has lack of interest in environment
Obtunded
What level of consciousness?
- Patient wakens only with painful stimuli. Verbal responses slow or absent. Falls back into unresponsive state when stimuli ceases
Stuporous
What level of consciousness?
- Patient is unarousable to any stimuli
Comatose
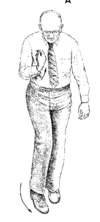
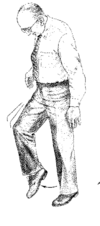
What posture is this?
–Upper extremities flexed at the elbows and held closely to the body
–Lower extremities are internally rotated and extended
Decorticate posture
___________
–Thought to occur when the brain stem is not inhibited by the motor function of the cerebral cortex.

Decorticate posture is thought to occur when…..

–Thought to occur when the brain stem is not inhibited by the motor function of the cerebral cortex.

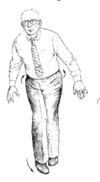
What posture is this?
- Rigid flexion;
- upper arms held tightly to side of body;
- elbows, wrists, and fingers flexed;
- feet are plantar flexed
- legs extended and internally rotated;
- may have fine tremors or intense stiffness
Decorticate

What is the site of lesion for decorticate posture?
corticospinal tracts, above the brainstem

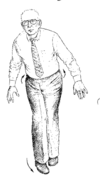
What posture is this?
–Seen in persons with extensive brain stem damage to the pons and lesions that compress the lower thalamus and midbrain
Decerebrate Posture

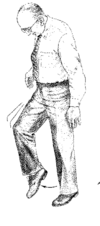
What posture is this?
- Rigid extension
- arms fully extended
- forearms pronated
- wrists and fingers flexed
- jaws clenched
- neck extended
- back may be arched
- feet plantar flexed
- may occur spontaneously, intermittently, or in response to a stimulus
Decerebrate

What is the site of lesion for the decerebrate position?
brainstem
3 questions of Orientation?
- Name
- Day or date
- Where are we?
Assessing speech and language. You are assessing:
- Talkative or silent?
- Does the patient speak spontaneously or only when directly questioned?
What aspect of speech and language is that?
Quantity
Assessing speech and language. You are assessing:
- Is the speech too fast, too slow, or just right?
What aspect of speech and language is that?
Rate
Assessing speech and language. You are assessing:
- Is the speech too loud, too quiet, or just right?
What aspect of speech and language is that?
Volume
Assessing speech and language. You are assessing:
- Can you understand what the patient is saying physically? If not, why not?
What aspect of speech and language is that?
Articulation
Assessing speech and language. You are assessing:
- Is the rate, flow, melody, and content of speech within normal limits?
What aspect of speech and language is that?
Fluency
Assessing speech and language:
If the rate, flow, melody, and content of speech are not within normal limits, what should you suspect?
If not, suspect an aphasia.
Speech and Language/Fluency
What are you testing?
- Ask patient to follow one or two step command
Word comprehension
Speech and Language/Fluency
What are you testing?
- Ask patient to repeat, “No ifs, ands, or buts”
Repetition
Speech and Language/Fluency
What are you testing?
- Ask patient to name the parts of a watch
Naming