Neuroimmunology Flashcards
(42 cards)
Behind trauma what is the leading cause of neurological disability in young ppl?
MS
Lesions of what location are most frequently the cause of noticeable disability in MS pts?
Spinal cord = major reason for disability in MS pts
How are MS attacks treated?
glucocorticoids- high dose given IV
How are severe MS attacks treated?
plasmaphoresis
What feature of exacerbation is associated w/ poor recovery and permanent disability
Inflammatory damage to myelin can also damage the underlying axon -axon damage is associate w/ poor recovery and permanent disability
What are the two most common disease modifying agents used in MS?
-interferon beta -glatiramer acetate -first line for most, safe/old drugs, but are injections
What is natalizumab?
Monoclonal antibody used as a disease modifying agent in MS -prevents lymphocytes from crossing the blood brain barrier -side effect = PML = progressive multifocal leukoencephalopathy
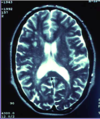
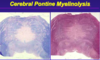
What is PML?
Progressive multifocal leukoencephalopathy = severe demyelinating CNS disease caused by reactivation of the JC virus
What can cause PML?
Duationof treatment w/ natalizumab (monoclonal anitbody for MS)
Besides acute treatment and disease modifying agents, what else can be done for MS pts?
Treat the physical, cognitive, and social disability Secondary meds to treat the fatigue, walking difficulties, ED, depression etc
What is the hallmark clinical finding of limbic encephalitis?
Short-term memory loss
What is limbic encephalitis?
inflammatory disorder of the limbic disorder
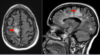
What is found in imaging of limbic encephalitis?
Hyperintensity of bilateral mesial temporal lobes

What are the clinical features of limbic encephalitis?
(recall: video of pt in Giant’s shirt who couldn’t remember Giants won the superbowl) -hallmark = short-term memory loss -psychiatric symptoms (hallucinations, delusions, psychosis, agitation), sleep disturbances, involuntary movements, autonomic dysfunction, seizures
What are some causes of limbic encephalitis?
LE divided into infectious and autoimmune causes -infectious often caused by viruses (ex: herpes simplex) -autoimmune often paraneoplastic: due to antibody production in association w/ a tumor
What is crucial to do when a pt is diagnosed w/ LE?
Limbic encephalitis- need to look for (to rule out or remove) tumor -removal of tumor can be curative -lots of LE cases can be paraneoplastic (due to antibodies produced in association w/ a tumor)
What is the treatment for LE?
-find a remove primary tumor -immuntherapies: IVIG, plasmaphoresis, steroids, monoclonal antibodies
What is NMO?
Neuromyelitis optica = Devi’s disease -inflammatory disease presenting w/ pathology of the optic nerve/chiasm, spinal cord, or brainstem
Differentiate the epidemiology of MS and NMO (a) gender disparity (b) racial disparity
MS (multiple sclerosis) vs. NMO (neuromyelitis optica) epidemiology (a) MS: M:F is 2:1, while NMO M:F is 10:1 (so NMO much much more common in females, but both are more common in F than M) (b) MS more common in whites, NMO more common in African American
How to diagnose NMO
1st- do blood test to test serum for NMO-IgG (seropositive in 75% of cases) -other 25% of cases (who are NMO-IgG seronegative) have 1 core clinical characteristic (w/o a better explanation): optic neurtis, acute myelitis, area postrema
What is Devic’s disease
NMO = neuromyelitis optica
What are the presenting features of Devic’s disease?
Loss of vision (either color, acuity etc) and SC fxn Presentation of SC dysfxn = muscle weakness, reduced sensation, loss of bladder/bowel control Typical pt: acute and severe spastic weakness of legs w/ sensory signs and loss of bladder control
Differentiate the MRI findings of MS and NMO
MS- shows small discrete plaques on MRI NMO- massive (like 3 vertebral bodies long) inflammatory lesions (much larger lesions, not small white dots)
Compare and contrast treatment for MS and NMO
Similarities- treat both MS and NMO attacks w/ steroids (and plasmapharesis if severe) Difference: disease modifying agents (interferon beta and glatiramer acetate) work in MS, but have no role against NMO