OSPE - Pathology tutorial pictures Flashcards
(74 cards)

New Epidermis on the top



What type of healing and label


What type of healing?

Secondary Intention:
- closure of the wound edge isn’t possible and a large deficit is present.
- additional step with wound contraction. Modified fibroblasts termed myofibroblasts contract, reducing the size of the deficit to be replaced
What’s this?

Keloid - overgrowth of scar tissue. Overgrowth of collagen.
Overgrowth of scar tissue is ‘proud flesh’ - looks different

What’s happened here?

Wound dehiscence in a failed primary closure
dehisce = (of a pod or seed vessel, or a cut or wound) gape or burst open:

P = periosteum
C = cortical bone (lamellar bone)
O = osteocytes in lacunae
H = haversian canal




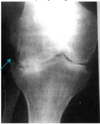
What’s going on here?

Non-union (bone ends are too far apart, fibrous union is when bone ends are joined by fibrous tisseu and bone’s failed to from) of femoral shaft following internal fixation
What’re these two conditions and what’re the common features seen?

Acute meningitis and acute appendicitis
Can see:
- vasodilation and congestion
- redness
- pus associated with meningitis
What’s this? And what can you see going on?

Subarachnoid space - congested vessels, background of stringy proteinaceous exudate and neutrophils
That vessel - dilated and lots of cells around - mostly neutrophils


This is a close up of the subarachnoid space in the brain. Normally this contains clear fluid and a scant number of cells
What’re the signs of acute inflammation seen in this photo?

Swelling, redness and pus
It’s actually carbuncle: a severe abscess or multiple boil in the skin, typically infected with staphylococcus bacteria (staph aureus)
Vessel that shows acute inflammation
- what are the cells lining the vessels?
- what’s the organisation of these cells?
- what adhesion molecues are involved?


How will these leisons heal?

Primary intetion - the skin edges are placed in close proximity. If you leave it like the one on the left, you’ll get a big scar
- How will this type of wound be treated?
- What options could be considered?


Label what you can

Wound contraction by myofibroblasts


The middle part - hard callous bc bone comes up pink

Name the tissues X, Y, Z and the cells a and b

X is cartilage because open tissue and grey/blue with frog eyes so those are chondrocytes/blasts

What cells are responsible for producing new bone?
Pluripotent cell derived from periosteum and bone marrow
5 months later - what’s happened?

Non union has occured - they haven’t healed together (bone ends too far apart)
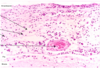
What is this a histology preparation from? What’s S and T?
What’s the diagnosis?
What’re some of the reasons that this has occured?
5 months later, still bad - what’re you gonna do?

From area of non union. S is fibrous connective tissue and T is woven bone. This is fibrous non union:
- Okay, so this is fibrous (mal)union - fibrous tissue connects the bone ends. Misalinged union of fracture by fibrous tissue. Surgery required to correct alignment and remove the fibrosis tissue. Bone grafting used to reproduce the haemotoma and start the healing process
- Non union is just wheh the bones are too far apart so probably dont get FCT?
Reasons it has happened:
- Excessive movement
- Not enough movement
- Infection
- Poor blood supply
- Poor nutrition
- Medications
After 5 months: reoperate and debride the connective tisse and create a new soft callus
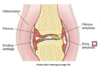
Label
What condition is this?

Rheumatoid Arthritis