congenital anamolies of pancreas
o Accessory (ectopic pancreas): pancreatic tissue outside it’s normal location (often in stomach, small intestine, meckel’s diverticulum)
o Annular pancreas: abnormal ring of pancreas that encircles the duodenum; assoc w/ down’s syndrome
o Pancreas divisum: failure of dorsal and ventral buds/ducts to fuse leading to retention of 2 separate duct systems; duct of santorinin provides main drainagel may cause acute pancreatitis
acute pancreatitis
common etiology
histo
Common etiologies: alcoholism, gallstones, mumps
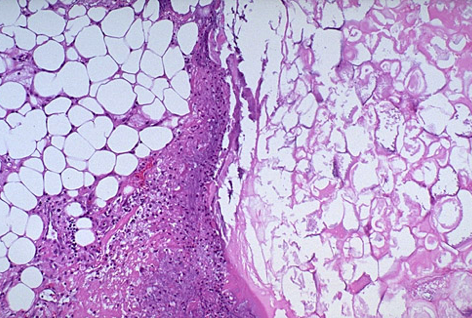
Hist:
- Edema by microvascular leakage
- Fat necrosis by lipolytic enzymes (saponification)
- Acute inflammation (neutrophils)
- Proteolytic destruction of pancreatic parenchyma
- Destruction of blood vessels and subsequent interstitial hemorrhage
Pic shows Fat necrosis with dystrophic calcifcation
acute hemorrhagic pancreatitis
o Abrupt onset following heavy meal/alcohol
o Extensive tissue destruction w/ circulatory collapse and shock
o Elevated serum amylase and lipase
o 50% mortality
o may develop pseudocyst
What type of pancreatitis?
Chronic
oRecurrent, progressive pancreatic tissue destruction
o Alcohol abuse is major cause
o Chronic inflammation, fibrosis, calcification
o Pancreatic insufficiency w/ malabsorption and/or diabetes
o 3-4% mortality/year
autoimmune pancreatitis
o 40s-60s
o assoc. w/ autoimmune conditions (PSC, Sjogren)
o some w/ multifocal inflammatory fibrosclerosis (Reidel thyroiditis, orbital pseudotumor, mediastinal and retroperitoneal fibrosis)
o mimics pancreatic carcinoma both clinically (obstructive jaundice) and radiologically (mass-like lesion)—“sausage-like” appearance on imaging
o elevated serum IgG4
o respond well to steroids
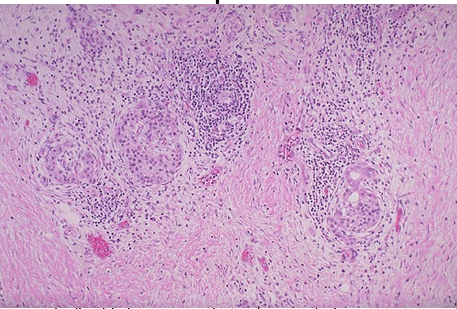
o Histo:
• Dense “duct-centric” inflammation of predominantly lymphoplasmacytic cells and expansion of periductal fibrous tissue
• Periphlebitis and obliterative venulitis common
• Interstitial fibroblastic proliferaion w/ storiform architecture
• IgG4+ plasma cells
hereditary pancreatitis
o AD, mutations in PRSS1 and SPINK1 result in autoactivation of trysinogen
o Same features of chronic pancreatitis except earlier age onset, less pancreatic calicification, and DM
o 40% develop pancreatic ductal adenocarcinoma
pancreatic ductal adenocarcinoma
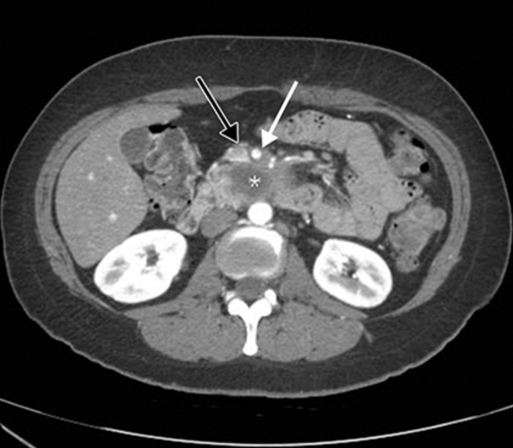
CT:
Most lethal solid tumor; Highest incidence after age 60
- o Risks: smoking, chemical exposure, high meat/fat diet, diabetes, chronic pancreatitis
- o KRAS activating mutations; Tumor suppressor mutations in p16, TP53, SMAD4
- o Precursor to cancer: pancreatic intraepithelial neoplasia
- o Sx:
- • Anorexia, wt loss
- • Abdominal/back pain
- • Jaundice
- • Migratory thrombophlebitis (troussea’s sign)—hypercoagulability and tendency to venous thrombosis
- o Derived from ductal cells; spreads by lymphatics and along nerves
- o 5 year survival=5% (only 20% are surgical candidates)
- o Gross: firm, gray poorly demarcated mass. Invasion of peripancreatic tissue and local structures common
- o Microscopic: >75% are well-moderately differentiated, prominent desmoplastic rxn, perineural invasion
pancreatoblastoma
o Children!
o Micro: acini and sqaumoid corpuscle
o 1/3 lymphn node/hepatic mets
pancreatic neuroendocrine neoplasms
o Derived from islet cells; non-functional or functional; M & F equally; ages 30-60; MEN1 syndrome
o Insulinoma (Beta-cell tumors): most common islet cell tumor
• Excess secretion of insulin→hypoglycemia, sweating, nervousness, hunger, confusion, lethargy
• Most are benign, solitary, small
• Uniform nests of cells, richly vascular, amyloid deposition
o Gastrinoma: G cell tumor secretes excess gastrin
• Zollinger-Ellison Syndrome (intractable gastric hypersecretion, peptic ulceration, and elevated blood gastrin levels)
serous cystadenoma
o Female predominance; pts with VHL at inc. risk
o Always benign, surgery is curative
o Composed of glycogen-rich cuboidal cells surrounding small (1 to 3 mm) cysts containing clear, thin, straw-colored fluid
mucinous cystic neoplasm
o Women
o Body or tail pancreas
o Painless, slow growing mass
o 1/3 assoc. w/ invasive carcinoma
o The cysts are lined by columnar mucinous epithelium, and a dense ovarian-type stroma
o Not involving the major pancreatic duct
intraductal papillary mucinous neoplasm
o Precursor to PDA
o Men
o Multifocal
o Can involve man pancreatic duct
o Lack ovarian type stroma
solid pseudopapillary neoplasm
o Low grade malignant neoplasm, 15% get mets
o Women in 20s
o Sx: intra-abdominal mass, palpable on exam
o Activating Mutation in beta-catenin
o cystic areas filled w/ hemorrhagic debris,
o Histo: cells as solid sheets, pseudopapillary,
cholelithiasis
o Gallstones in gallbladder or extrahepatic biliary tree
o Asymptomatic but may present w/ pain (biliary colic) if in cystic or common bile duct and fatty food intolerance
cholesterol stones
o Yellow-tan; cholesterol calcium salts, mucin; radiolucent
o Risks: women of reproductive age, inc. age, obesity, ethnicity, diet, metabolic abnormalities, drugs
o Contributing factors (4)
• Hypersaturaiton of bile w/ cholesterol
• Gallbladder hypomotility
• Crystal nucleation accelerated
• Hypersecretion of mucus in gallbladder traps crystals leading to aggregation
black pigment gallstones
o calcium bilirubinate, calcium salts, mucin; radioopaque
• Inc. conc. of unconjugated bilirubin in bile—chronic hemolysis, cirrhosis
brown pigment stones
calcium bilirubinate, cholesterol, calcium salts, fatty acids; radiolucent
- Bacterial cholangitis (E. coli), biliary heminthic infection, mechanical obstruction of bile flow (PSC)
- More often found in bile ducts than gallbladder itself
acute cholecystitis
o Diffuse inflammation of gallbladder 2/2 obstruction
o 95% assoc. w/ gallstones
o Acalculus cholecystitis: sepsis, severe trauma, polyarteritis nodosa, salmonella infection
o Gross:
• Gallbladder enlarged and tense; bright red or blotchy, violaceous to green-black discoloration, imparted by subserosal hemorrhages
• serosal covering is frequently layered by fibrin and, in severe cases, by suppurative exudate
• lumen may contain stones, is filled with a cloudy or turbid bile that may contain large amounts of fibrin, pus, and hemorrhage
• wall is thickened, edematous, and hyperemic.
• Perforation (bile peritonitis)
o Microscopic:
• Acute inflammation and edema
• Hemorrhage of the gallbladder wall
• Mucosal ulceration or widespread necrosis (gangrenous cholecystitis)
chronic cholecystitis
o Persistent inflammation of gallbladder
o >90% associated with gallstones
o Gallbladder has thickened and fibrotic wall
o Rokitansky-Aschoff sinuses
o Gross:
• Wall is thick and firm 2/2 extensive fibrosis
• Gallstones in lumen
• Mucosa ulcerated and atrophic or intact
o Microscopic:
• Wall is fibrotic w/ prominent R-A sinuses
• Chronic inflammatory infiltrate
• Long standing inflammation→calcification (porcelain gallbladder; inc. risk cancer)
Cholesterolosis
accumulation of cholesterol-laden macrophages in submucosa of gallbladder
o Gross: prominent scattered yellow flecks, strawberry gallbladder
gallbladder adenocarcinoma
• Carcinoma: adenocarcinoma of gallbladder assoc. w/ cholelithiasis and chronic cholecystitis
o F>M
o >50yo
o RUQ abdominal pain, anorexia
o Metastatic disease
o Gross: diffuse wall thickening or polypoid growth
o Histo: adnocarcinoma w/ varying degrees of differentiation
Normal Pancreas. Compare to what is shown on the back.
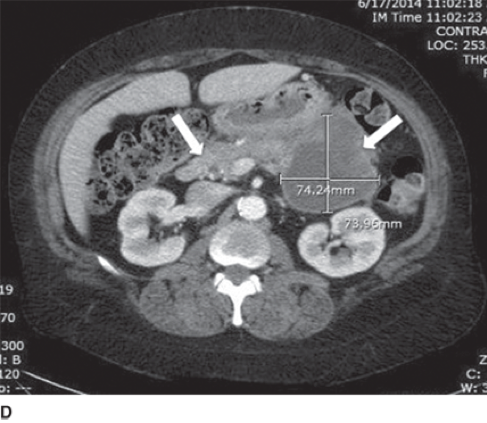
Pseudocyst
Causes of acute pancreatitis:
GET SMASHED
G: Gallstone
E: Ethanol
T: Trauma
S: Steroid
M: Mumps
A :Autoimmune
S: Scorpionbites H: Hyperlipidemia E: ERCP
D: Drugs
Dx tools
X-ray
CT
US
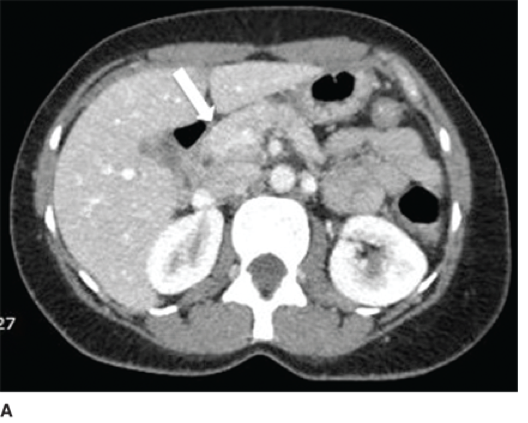
CT of abdomen:
- •Estimates severity and prognosis
- •Complications include phlegmons, abscesses or pseudocysts.
- •Usually seen 2-3 weeks after acute pancreatitis
•Xrays of chest/abdomen: useful for r/o other diagnosis.
- •Calcification of pancreas with chronic pancreatitis
- •May see sentinel loop, elevated hemi-diaphragm, pleural effusion
- •
• U/S: may detect gallstones


