Pharm: Opioids Flashcards
(44 cards)
Which opioid agonist is used for pulmonary edema?
Morphine
Which 2 opioid agonists are used for severe pain and as an adjunct in anesthesia?
- Fentanyl
- Morphine
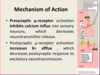
What is the MOA on both the presynaptic μ-receptor and post-synaptic μ-receptor by opioids?
- Presynaptic μ-receptor activation INHIBITS Ca2+ influx into sensory neurons, which decreases NT release
- Post-synaptic μ-receptor activation INCREASES K+ efflux, which decreases postsynaptic response to excitatory neurotransmission
What are the 3 opioids which are strong μ-receptor agonists?
- Morphine
- Fentanyl
- Methodone
What are the pharmacokinetics of the strong opioid agoinsts?
Exception?
- First pass effect
- Duration 1-4 hours
- Except methadone = 4-6 hours
What’s the MOA of Codeine and Hydrocodone, as compared to the strong opioid agonists?
- Less efficaious than morphine, partial μ-receptor agonists
- Can antagonize strong agonist
What are the clinical applications of Codeine and Hydrocodone?
- Mild-moderate pain
- Cough (codeine)
What are the 2 opioids belonging to the class of mixed opioid agonist-antagonist?
- Buprenorphine
- Nalbuphine
What are effects of the opioids, Buprenorphine and Nalbuphine?
- Like strong agonists, but can antagonize their effects
- Also reduces craving for alcohol
What is Buprenorphine used for clinically?
- Moderate pain
- Some maintenane rehabilitation programs
What is the duration of action for Buprenorphine and Nalbuphine and associated toxicity?
- Long duration of action: 4-8 hours
- May precipitate abstinence syndrome
What is the clinical application for the use of the opioid, Nalbuphine?
Moderate pain
What is the effect of Dextromethorphan?
- Reduces cough reflex
- Not an analgesic
What is Dextromethorphan used for?
Acute debilitating cough
*This is Nyquil or Robitussin = Antitussives
What is the MOA of Naloxone?
Strong antagonist of μ, δ, and k receptors
What is clinical application for Naloxone?
Opioid overdose
What is a potential toxicity associated with Naloxone?
Precipitates abstinence (withdrawl) syndrome in dependent users
What is the MOA of the analgesic, Tapentadol?
- Moderate μ agonist
- Strong NET inhibitor
What is Tapentadol used for clinically?
Moderate pain
What are some of the toxicities/consequences associated with Tapentadol?
- Headache; nausea and vomiting
- Possible dependence
What is the MOA of the analgesic, Tramadol?
- Weak μ agonist
- Moderate SERT inhibitor
- Weak NET inhibitor
*Mixed effects
What is the clinical application of Tramadol?
- Moderate pain
- Adjunct to opioids in chronic pain syndromes
What are some of the potential toxicities associated with Tramadol?
- Seizures
- Risk of serotonin syndrome
What is the MOA of Naltrexone and Nalmefene; how are they different from Naloxone?
- Strong antagonist of μ, δ and k receptors (just like Naloxone)
- Longer duration of action (10 hours!)









