Recon Flashcards
(424 cards)
What is the most common cause of early revision in hip resurfacing?
periprosthetic fracture
most common
What linear wear rate has been associated with osteolysis and loosening?
> 0.1 mm/year
5 variables leading to PE wear characteristics
PE thickness:
- should be >8mm
Articular surface design:
- higher congruity/contact surface area leads to lower contract stress and better wear characteristics
Kinematics:
- ie knee kinematics. Change them to get most congruous implant
PE sterilization:
- Gamma radiation Sterilization in oxygen depleted environment is best
- Then package in vacuum, argon or nitrogen environment
PE machining
- Best is with direct-compression molding
4 complications of free fibula vascularized bone graft?
- sensory deficit
- motor weakness
- FHL contracture
- tibial stress fracture from side graft is taken
5 Considerations in sickle cell in arthroplasty
Pre-op
Check for osteomyelitis
Avoid sickle cell crisis (lots of fluids, oxygenate, avoid acidosis)
CHF often present with chronic anmeia
pre-op transfusion/plasmaphoresis
Intraop
Protrusio
Widened canal (marrow hyperplasia)
poor bone quality
osteonecrosis
Postop
Higher infection rates (no salmonella)
Do NOT need to cover for salmonella
Higher rates of dislocation
Techniques to reduce nerve injury in THR for DDH?
- good pre-operative planning
- limb lengthening
- subtrochanteric osteotomy
- intra-operative wake-up test
- neurophysiologic intraoperative monitoring
- downsizing implant components if presenting with deficits peri-operatively
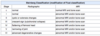
On an AP xray, what landmarks are most useful for assessing acetabular cup position?
- medial border of cup should approximate the ilioischial line and lie close to the teardrop
- inferior border of cup should be at level of inferior teardrop line
Postpartum female with hip pain - what do you think of?
transient osteoporosis of hip
5 ways to avoid failure of cemented femoral stem.
- smooth stem
- > 2 mm mantle
- rigid stem
- centralized stem
- No defects of mantle
Two main contraindications to hip osteotomy?
Restricted hip motion
Advanced OA
List 4 devices available for fixation of a TKA periprosthetic femoral fracture
condylar buttress plate (non-locking)
locking supracondylar plate
blade plate
dynamic compression screw
Most common nerve injury with hip scope?
Pudendal from traction
Describe femoral rollback
Lateral condyle has a larger curvature of radius so as you flex & extend the knee, the lateral condyle will pivot about the medial side
Conceptually, what is the ideal patient to use constrained components in THA?
In patients with a soft tissue insufficiency not amenable to repair or augmentation
it is NOT to correct for malalignment
Saggital balancing:
Flexion: Loose
Extension: Tight
What do you do?
resect femur + thicker poly
or
release capsule posteriorly and thicker poly
Differentiate adhesive, abrasive, and third body wear.
adhesive wear
most important in osteolytic process
microscopically PE sticks to prosthesis and debris gets pulled off
abrasive wear
cheese grater effect of prosthesis scraping off particles
third body wear
particles in joint space cause abrasion and wear
Indications for a hinged knee prosthesis?
- global instability
- massive bone loss in a neuropathic joint
- oncologic procedures
- hyperextension instability
3 benefits of increasing offset?
- increased soft-tissue tension
- decreased impingement
- decreased joint reaction force
Risks of patellar periprosthetic fracture
patellar osteonecrosis
asymmetric resection of patella
inappropriate thickness of patella
implant related
- central single peg implant
- uncemented fixation
- metal backing on patella
- inset patellar component
General workup algorithm for MoM patients
Yearly assessment (x-ray, blood levels)
If high risk: get advanced imaging (MARS MRI)
Revision if:
Symptomatic, osteolysis, poor cup abduction angle, increasing metal ion level, pseudotumour

5 risks of HO in TKA
Periosteal stripping of anterior femur
Male
Obesity
Post-traumatic
Hypertropic osteophystes preop
Arthropathy (DISH, AS)
Paget’s
Cementless components
Approach: iliofemoral > Kocher > II
Manipulation post op
(NOT RA)
in DDH THA, name 3 ways to decrease sciatic nerve palsy
Visualize/palpate for tension
lengthen 4cm or 15-20% of length (some say
Neuromonitoring
Risk factors for Hip OA
Modifiable
Articular cartilage
Muscle weakness
Heavy physical stress at work
High impact sporting activities
Non-modifiable
Female
Increased age
Genetics
Developmental/acquired deformities
Hip dysplasia
SCFE
LCP
2 ways of testing for nickel sensitivity?
- patch testing
- lymphocyte transformation test (LST)