Spotter Flashcards
What does this ECG show and why?

S-T depression, can be sign of chronic ischaemia
Label A-C

A: arcuate vessels
B: interlobular arteries
C: interlobar vessels
What are A, B and C?

A: posterior intercostal artery
B: lateral cutaneous branch
C: anterior intercostal artery
Label A-F around the diaphragm.

A: Aorta
B: R sympathetic trunk
C: L sympathetic trunk
D: Azygos
E: Thoracic duct
F: IVC
NB: diaphragm attachement around costal margin (inferior border of lower rib)
What changes can you see in this asthma-affected airway?

Mucous plugging
Wall thickening (inflammation)
Smooth muscle hypertrophy
What is wrong in this Xray?

Mitral valve stenosis, enlarged L atrium and pulmonary oedema.

What are the 2 main features of this CXR?

Batwing
Blunting of costophrenic angle. If fluid in pleural cavity, goes to this area due to gravity = indicitave of pleural effusion, can be caused by many things e.g. heart failure
Label A-C (with percentages)

A: plasma 55% (water 90%, solutes 10%)
B: erythrocytes (45%)
C: Leukocytes and thrombocytes (platelets)
What is this showing in the lungs and why?

Pulmonary TB
Early Mycobacterium tuberculosus - early caseous granuloma , central area of caseous necrosis (CN), surrounded by macrophages (M) which fuse to giant Langerhans cells (L). Arrows = rim of lymphocytes.
What type of ciliated epithelium is this?
What is the arrow pointing to?
What are the arrow heads pointing to?
Simple columnar
Smooth muscle
BALT
65yo male, increasing breathlessness on exertion, long history of diabetes mellitus and hypertension leading to poor renal function. Low Hb.
How would you best classify this patient’s anaemia?
What terms describe the red cell appearances?
What is the most likely reason for this patient’t anaemia?

Normocytic
Acanthocytes (burr cells), schistocytes (fragments), anisocytosis (diff shapes), poikilocytosis (diff sizes)
Erythropoietin deficiency. (Anaemia due to chronic renal failure and consequent EPO deficiency, anaemia usually normocytic with red cells showing abnormalities including spicules and “burr” cells. Red cell fragments may be seen with renal vascular disease).
What does this ECG show and why?

No P wave - atrial fibrillation (pacemaker cells firing at different times = asynchronised and no electrical activity)
What is B in the lung?

Bronchiole
What are the features on this CXR?

Pleural effusion (in e.g heart failure, lungs so saturated that fluid accumulates in pleural space. A step worse from pulm oedema.
Pulmonary oedema (fluid in intersitium)
Large cardiothoracic ratio
Chest wires
What can you see in this CXR and what does this suggest?

Visceral pleural edge, air in pleural cavity

Pneumothorax
Label A-D

A: pituitary stalk
B: hypothalamus
C: pituitary gland
D: hypothalamus
Label the parts of the sternum

A: Sternal angle
B: xiphoid process
C: manubrium
4: body
What are these structures?

Seromucous glands
What are A-F?
A: coronary sinus
B: fossa ovalis
C: tricuspid valve
D: chordae tendinae
E: papillary muscles
F: trabeculae carnae
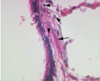
This is a longitudinal section of foetal trachea branching into the main bronchi. What is the tissue indicated by the arrows?

Hyaline cartilage
What do these CXRs show?

Pneumothorax - in 1) clearly see L lung pulled away from side, in 2) can see R visceral pleural edge
What does this CXR show? (Normal on L)

Hyperinflation - dyspnea
Identify the 3 lung cell carcinomas.

A: small cell carcinoma (small, ovoid and densely packed, dark stained, disseminate widely)
B: squamous cell carcinoma (large esinophill cells/central whorling)
C: Adenocarcinoma (G = gland)
What are A and B?

A: azygos vein
B: hemiazygos vein
What condition is this? Explain the colour.

Lobar consolidation.
Lower lobe shows lobar consolidation.
What has happened in this Xray?
List possible causes.

Pulled airways.
collapse of lobe, loss of lung volume, consolidation, fibrosis

Label the major and accessory muscles involved in inspiration, A-F

A: SCM
B: Pectoralis major
C: Rectus abdominis
D: Pec minor
E: Serratus anterior
F: External intercostal muscles
Comment on this ECG. What could have caused it?

AMI = STE: II, III, aVF. Blocked RCA.
Label A and B

A: basilic vein
B: cephalic vein
NB: deep veins take same name as arteries.
If body is A, remember it as A -> B -> C in anatomical position
Label A-F

A: Frontal sinus
B: ethmoid air cells
C: sphenoid air sinus /opening of
D: maxillary air sinus (opening of)
E: frontonasal duct
F: semi lunar hiatus
Label 1-6 of the femoral triangle.

- femoral artery
- femoral nerve
- femoral vein
- ASIS and lateral femoral cutaneous nerve
- inguinal ligament
- sartorius
Label A-D

A: superficial palmar arch
B: metacarpal artery
C: digital artery
D: deep palmar arch
NB. metacarpal and digital arteries arise from arches and supply fingers
Palmar arches: anastamoses of R and V arteries
What can you see in this CXR?
What is this caused in congestive heart failure?

Pulmonary oedema. Bat wings (bilateral perihilar shadowin due to fluid accumulation)
Heart unable to pump blood efficiently, blood can back up into veins that take blood through lungs. As pressure in these BV increases. fluid is pushed into alveoli in lungs, reducing normal O2 movement.
Identify A and B in the brochus

A: seromucus glands
B: hyaline cartilage
Describe the cell and possible diagnosis.

Hypersegmented neutraphils. Macrocytic anaemia - B12/folate deficiency
Label A-C
A: tunica intima
B: tunica media
C: tunica adventitia
Label A-D

A: pulmonary valve
B: aortic valve
C: mitral valve
D: tricuspid valve
Label A-E in blood cell development

A: myeloid SC
B: myeloblast
C: lymphoid SC
D: megakariocyte
E: lymphoblast
Label A-D

A: R. subclavian
B: brachiocephalic trunk
C: R and L common carotids
D: L. subclavian
What are A-F?

A: SVC
B: fossa ovalis
C: IVC
D: coronary sinus
E: tricuspid valve
F: pectinate muscle
What stage of these images is pulmonary TB? What can be seen?

Later TB. Fibroblasts lay down collagen in ECM to wall off tubercle.
A patient has had a troublesome cough for a year, brings up whitish sputum. What has happened to the mucus producing cells here? What condition causes this?

Hypertrophied.
Chronic bronchitis
Label A-D in the bronchus

A: pseudostratified columnar epithelium
B: lamina propria
C: muscularis mucosae
D: submucosa
Label A-C. What is happening?

A: endothelium B: hemorrhage C: plaque
Unstable plaque (still covered by endothelium)
Photomicrograph from conducting airway. What kinds of cells are A and B?

A: stratified squamous epithelium
B: pseudostratified columnar epithelium with goblet cells
(NB. B have become A due to metaplasia from smoking)
Label A-D
What is C sensory and motor to?
What are the contents of the carotid sheath?

A: Brachial plexus
B: Vagus nerve
C: Phrenic nerve
D: L recurrant laryngeal nerve
Sensory to the two membranes it’s inbetween: the mediastinal section of parietal pleura and pericardium. Motor to diaphragm.
IJV, carotid arteries, vagus (IC 10 CCs in the IV)
NB: phrenic starts more laterally and decreases to diaphragm. More anterior. Vagus starts in carotid sheath more posterior and continues to move posteriorly on L side next to oesophagus -> through osophageal hiatus (T10)
What is does this CT show?

Sinusitis - mucus accumulation. May have toothache and frontal facial pain.
Label A and B

A: internal thoracic artery
B: R. subclavian artery
Label A-D
What is this structure?
A: intermediate filament
B: dense body
C: mechanical junction coupling cells
D: gap junction for electrical and chemical communication
Smooth muscle
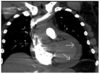
What is this image showing?

Aortic stenosis - calcifications on stenotic valve

Label A-F

A: horizontal fissure
B and C: oblique fissure
D: lobar bronchus
E: segmental bronchi
F: carina (sternal angle)
Determine whether A and B are PA or AP Xrays and why.

A: PA
B: AP because scapula lies over lung fields and clavicles are horizontal
Label A-C of this platelet.

A: lipid bilayer cell membrane, and glycoprotein receptors
B: dense body
C: alpha granule
17yo female, sore eyes, nasal discharge, eosinaphils raised.
What is the salient feature of the blood count and film?
What is the likely diagnosis?

Eosinophilia
Allergic rhinitis
What are A & B?

A: Internal intercostal muscle
B: External intercostal muscle
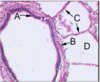
Label A-D in a conducting airway.

A: columnar cells
B: cilia
C: goblet cell
D: mucus
NB. in lower condicting airways (bronchioles), simple epithelium only. Epithelium EXCEPT ALVEOLAR is covered with mucus
Label Waldeyer’s ring, A-D.

A: adenoid
B: tubal tonsil
C: palatine tonsil
D: lingual tonsil
3yo male, vegetarian meal, became unwell, pink urine, favism diagnosis. Low Hb, high reticulocytes, heinz bodies seen on reticulocyte preparation (oxidised denatured Hb).
What are the salient features of his blood film (above)?
How would you best classify his anaemia?
What are the key factors leading to the development of this patient’s anaemia?

Polychromasia (high number of immature RBC), basket cells (bite/blister cells)
Non-spherocytic haemolytic anaemia
Glucose-6-phosphate dehydrogenase (G6PD) deficiency and ingestion of fava beans. (Most sig in Mediterraneans, sex-linked male inheritance, female carriers show half the normal G6PD cell value.
G6PD reduces NADP while oxidising glucose-6-phosphate. It’s the only source of NADPH in red cells and deficiency renders cell susceptible to oxidant stress. Deficiency usually asymptomatic, but in response to oxidant stress e.g. drugs, fava beans, or infections, acute haemolytic anaemia develops. Heinz bodies are formed in red cells in response to oxidant stress and are removed by the spleen, leading to acute intravascular haemolysis with haemoglobinuria. Heinz body removal leaves ‘basket’ or ‘bite’ red cells.)
Label the facia of the neck, A-D
What structures does B contain?

A: pretracheal fascia
B: carotid sheath
C: Prevertebral fascia
D: deep investing fascia
E: retropharyngeal space (between PTF and PVF)
common carotid artery, internal jugular vein, vagus nerve (VIC)
70yo female, increasing tiredness and breathlessness, recently constipated, pale.
What are the salient red cell features in this blood film?
How would you best classify the pt’s anaemia?
What is the most likely cause?
What is the likely diagnosis?
Pencil cells
Microcytosis
Hyperchromasia
Microcytic
Fe deficiency
Large bowel carcinoma
Label A-C in the alveoli

A: Type 1 pneumatocyte
B: Type 2 pneumatocyte
C: Alveolar macrophage (b/c mucus would compromise gas exchange, so no mucus but macrophages instead)
What is this muscle?
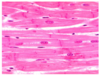
Cardiac
What type of cells are P1, P2 and M?

P1: type 1 pneumatocytes
P2: type 2 pneumatocytes
M: macrophage
Label D, 6, 7, 9 and 11

D: juxtaglomerular apparatus
6: granualar cells (juxtaglomerular cells)
7. macula densa
9. afferent arteriole
11: efferent arteriole
Label A-E

A: superior cervical sympathetic ganglion
B: Cervical sympathetic trunk
C: Vertebral artery
D: Middle cervical ganglion
E: Inferior cervical ganglion
What does this ECG show and why?

S-T elevation = acute ischaemia (but most common cause = AMI)
Identify the components of the adult trachea shown.

- epithelium
- seromucus glands
- lamina propria/submucosa
- hyaline cartilage
- adventita
Label A-D

A: tricuspid valve
B: mitral valve
C: aortic valve
D: pulmonary valve
Label A-C of the larynx during rest

A: vestibular fold - choking reflex
B: Rima glottidis - aperture
C: vocal fold - contain vocal ligament and vocalis muscle
Label A-C and explain the function of A and B

A: metarteriole
B: throughfare channel
C: precapillary sphincter
A and B = vascular shunt, arteriovenous anastomoses, flow through capillary bed can be shut off and blood goes directly through from arteriole -> venule
64yo male, 3 day history of fever, sweating, vomiting and rigors, recently returned from trip to uganda. Platelets and Hb low.
What diagnostic feature is present on the blood film?

Malarial parasites in red cells. (Some degree of haemolysis seen in all types of malaria. Thrombocytopenia is commonly found in acute malaria. Reticulocytosis is usually present in the face of haemolysis but this is often absent in the face of overwhelmind sepsis.)
What has happened in this Xray?
List possible causes.

Pushed airway
Masses, tension pneumothorax

What are A,B and C?

A: jugular notch
B: costal cartilages
C: costal margin
What does this Xray show and what could have caused it?

Blunted costophrenic angle (L and R)
Can be caused by fluid in pleural cavity - pleural effusion
Label A-D

A: L recurrant laryngeal
B: Vagus
C: phrenic
D: azygos vein
The nerves are anterior to the lung root.
19yo med student, sore throat, friend recently had glandular fever, temp 39 degrees and tonsils inflammed with pustular exudate. HIgh neutrophil levels (neutrophilia).
What is the likely cause of this pt’s sore throat?

Bacterial infection (glandular fever is caused by Epstein Barr virus so would cause other alterations in blood results)
Label A and B. What is does A do?

A: catrotid body B: carotid sinus
Label A-C. ECG leads vaguely correspond to areas of the myocardium supplied by the coronary arteries. Label which ones.

A: LCx or diagonal branch of LAD
B: RCA or LCx
C: LAD
Label tissues A and B in the lungs

A: Respiratory epithelium: ciliated psudostratified columnar with goblet cells
B: Bronchus associated lymphoid tissue (BALT) in lamina propria
What types of cells are A and B?

A: Multiunit SM cell
B: Single unit SM cell
What is this muscle?

Smooth
What do the P,Q,R,S, and T waves show?

P: atrial depolarisatin
QRS: ventricular depolarisation
T: due to differences in time of ventricular repolarisation
Label A-C. What has happened in this post-mortem?
A: post mortem blood clot
B: thrombus
C: atheromatous plaque
Thrombus has formed on plaque surface
What is this condition?

DVT
What does this ECG show and why?

Extra P waves - atrial flutter (look at V1), often due to poor blood supply to SAN
Label 1-10

1: trachea
2: hilum
3. lungs
4. diaphragm
5. heart
6. aortic knuckle
7. Ribs (P and A)
8. scapulae
9. breasts
10. stomach
Label A.

Posterior intercostal artery, directly from aorta, most blood in intercostal spaces comes from it.
Label A-D

A: Extraglomerular mesangial cells
B: Macula densa cells
C: Granular cells
D: juxtaglomerular apparatus
Label A-H

A: afferent arteriole
B: DCT
C: macula densa
D: juxtaglomerular cell
E: efferent arteriole
F: bowman’s capsule
G: glomerulus
H: PCT
What does this ECG show and why?

Ventricular fibrillation - grossly abnormal ECG with no clear QRS complexes
Label A-C

A: Lateral plantar artery
B: plantar arch
C: medial plantar artery
Label A-F

A: gap junction
B: intercalated disc
C: sarcoplasmic reticulum
D: A band (thick)
E: I band (thin)
F: Z disc
Label the parts of the pharynx

A: nasopharynx
B: oropharynx
C: laryngopharynx
D: oseophagus
What has happened here (L = normal lung histology)? Collagen stained blue.

R = pulmonary fibrosis. Restrictive respiratory disease.
What is this line?

Visceral pleural edge
Label A-C in the lungs

A: ciliated cell
B: goblet cell
C: connective tissue
What is this condition?

Post-thrombotic syndrome
Label A-C

A: Superior vena cava
B: azygos vein
C: hemiazygos vein
What do you see here? What condition is this? (Normal lung = left)

Loss of acinar structure
Emphysema
Label the parts of the larynx, A-G

A: hyoid: C3, free-floating bone, anchoring point
B: thyroid cartilage
C: laryngeal prominance
D: cricoid cartilage - C6, only cartilage forming complete ring around trachea
E: thyroid isthmus
F: tracheal rings
G: thyroid gland
What are A, B and C?

A: Phrenic nerve
B: Vagus nerve
C: Recurrant laryngeal nerve
What can you observe here?

Metal wires from cardiothoracic surgery (top arrow)
Valve replacement (bottom arrow)
In aorta- breakdown of epithelial cell wall, get pale lumen, aorta swollen with blood,
Label cells A-E

A: neutrophil
B: eosinophil
C: basophil
D: monocyte
E: lymphocyte
Label A-F

A: mitral valve closes
B: aortic valve opens
C: aortic valve closes
D: mitral valve opens
E: isovolumetic contraction
F: isovolumetric relaxation
What is unusual about this patient?

Cervical ribs.
May cause problems e.g. impinge on brachial plexus
What can you see in this CXR?

2 pleural effusions
Label A-D in the lung
A: epithelium
B: muscularis mucosae
C: interalvolar septa
D: alveolus
Label A-C

A: septal cartilage
B: perpendicular plate of ethmoid
C: vomer
What lung condition is shown here? What is indicated by the letters and arrows?

Tuberculous bronchopneumonia
B: bronchial wall (containing infected material)
D: Where mycobacteria have destroyed part of the wall
T: tubercle in adjacent tissue
Label A-H

A: opening of superior vena cava
B: tricuspid valve
C: myocardium of R ventricle
D: papillary muscles
E: mitral valve
F: chordae tendinae
G: interventricular septum
H: myocardium of L ventricle
Label cell A. What is happening in B?

A: platelets
B: platelets budding off
Label A-C

A: Continuous capillary
B: Fenerstrated capillary
C: discontinuous/sinusoidal capillary
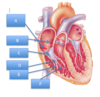
What are A, B, C, D and E?

A: R. atrium
B: R. ventricle
C: L. ventricle
D: Pulmonary trunk
E: ligamentim arteriosum
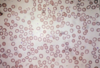
What kinds of cells are indicated by the arrows?

Reticulocytes
Label the 3 layers of chest wall muscles that help move the ribs, and describe their properties.

A: Innermost intercostal - deficient posteriorly - same as internal
B: Internal intercostal - go in opposite direction to external
A & B act as unit.
C: External intercostal - ends anteriorly at mid-clavicular line, forwards and downwards orientation, contract = pull ribs up
What do these lungs display?

Large bullae - increase in air spaces = emphysema
What is the problem?

No common iliac on the right!! (L side - normal)
Label what A-C show

A: a wave - atrial contraction before tricuspid valve closes
B: c wave - pressure rising in atrium just after tricuspid closes b/c valve bulges back into atrium
C: v wave - venous filling when tricuspid valve is closed
What can you see in this blood film, and what is a possible diagnosis?

RBCs oxidised and damaged, haemolytic anaemia
What type of cell is shown here?
What is the greyish substance the arrows are indicating in the upper part of some of the cells?
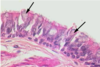
Goblet cells
Mucin
What can you see in this before and after angiogram?

RCA almost occluded before. After = stented
What can you see in this abdominal aorta?

Plaques all over endothelial layer. Has had bifurcation replaced. Huge aneurysm.
Label the coronary blood supply

A: L. coronary artery
B: R. coronary artery
C: mitral valve
Label A and B.
Where do they project to?

A: supraoptic nucleus B: paraventricular nucleus
Project to post pituitary gland
What are A - G?

A: auricle of LA
B: L ventricle
C: coronary sinus
D: PIG (post. interventricular groove)
E: R. ventricle
F: L. atrium
G: L pulmonary arteries
35yo city banker, lethargy, poor appetite, well-nourised, large tender liver. High MCV, low platelets.
From the pt’s blood count (above) what are the main abnormalities?
What are the salient features of the pt’s blood film?
What is the likely diagnosis?

Macrocytosis, thrombocytopenia (low blood platelet count)
Macrocytosis, thrombocytopenia, target cells (dark ring surrounding dark central spot)
Alcoholic liver disease (alchohol is most frequent cause of raised MCV in the absence of anaemia. Macrocytosis is often accompanied by the presece of target cells, mainly as a result of increased cholesterol in the red cell membrane. Thrombocytopenia commonly occurs with excessive alcohol intake. Folic acid deficiency may be an additional cause of macrocytosis in poorly nourished alcoholic pts.)
Label A-E

A: Circumflex
B: AVN (supplied by RCA)
C: LAD
D: Posterior (interventricular) descending
E: RCA
F: right marginal
Label A-C

A: Ulnar artery
B: Radial artery
C: Common interossus
Label A and B

A: foramen ovale
B: ductus arteriosus
Label A-G

A: RCA (emerges from aortic sinus)
B: Posterior (interventricular) descending
C: Right marginal
D: LCA (1-2 cm long, divides into E and G)
E: L circumflex
F: L marginal
G: LAD
What can you see in this CXR?

Massive pleural effusion.
Due to heart failure prob.

What are A, B, C, D and E?

A: Endocardium
B: Myocardium
C: Epicardium
D: Atrioventricular valve
E: Branch of the coronary artery
Label A and B.

A: brachial artery
B: profunda brachii
Label A-D, the optimal stethoscope positions for hearing different sounds.

A: aortic semilunar
B: pulmonary semilunar
C: left AV
D: right AV
What can you see in this CXR?

Tension pneumothorax: pressure in pl cavity increases, cause cardiogenic shock b/c lung collapses onto mediastinum, and it shifts. See the trachea pushed to one side.

What has happened to these alveoli? (Normal on L)

Emphysema on R - grossly enlarged alveoli (bullae).
Lung volume isn’t decreased so not a restrictive disease, but compromised O2 transpot in b/c has longer distance to diffuse -> can suffer chronic hypoxemia and hypercapnia.
Label A-F

A: soft palate
B: uvula
C: Palatine tonsil
D: palatoglossus
E: palatopharyngeus
F: posterior wall of oropharynx
What does this patient have and why? What are the triad of main sysmptoms?

Horner’s Syndrome - sympathetic fibres stretched/damaged along course to head/neck. If unilaterally disturbed, get triad of main symptoms:
- Partial ptosis (paralysis of superior tarsal muscle)
- Miosis (constriction of pupil die to paralysis of dilator pupillae)
- Anhydrosis (decreased sweating affecting same side of face as leision due to loss of facial sweat gland innovation)
What is this?
Pericardial effusion leading to pericardial tamponade
What condition is this?

Bronchopneumonia
Peribronchal foci of consolidation centre on small bronchi and bronchioles that show evidence of acute purulent bronchitis (P)
What condition is this?

Kwashiorkor - severe malnutrition -> protein deficiency in blood and tissues -> decreased OPc, pitting oedema and water retention in gut.
Label A-C

A: cardiac plexus
B: pulmonary plexus
C: eosophageal plexus
50yo male, increasing breathlessness, dark urine, yellow appearance, pale and icteric. Low Hb, high reticulocytes and WBC, normal MCV.
What are the salient features of his blood count (above)?
What are the imporant features seen on the blood film?
What term best describes his anaemia?

Reticulocytosis, neutrophilia, normocytic anaemia
Polychromasia (reticulocytosis), nucleated red cell (erythroblast), spherocytes
Spherocytic haemolytic anaemia. (He has classic features of haemolytic anaemia:
1) increased red cell break down (raised serum unconjugated bilirubin and excess urinary urobilinogen)
2) increased red cell production
3) red cell damage (spherocytosis) - either inherited or immune, and since the pt has not been anaemic before, this must be autoimmune haemolytic anaemia)
Label A-C

A: Aorta
B: Inferior vena cava
C: Oesophagus
What is happening at A, B & C in this ventricular muscle AP?
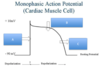
A: Na+ enters cell, depolarisation
B: Ca2+ enters cell, contraction initiation
C: K+ exits cell, repolarisation
Smoking and Chronic Bronchitis
Normal respiratory epithelium is on the left. What is to the right?
Name the process that has occured.
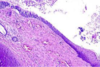
Stratified squamous
Metaplasia
Label A and B in this coronal CT scan.

A: maxillary sinus
B: ethmoid sinus
Label A-D

A: podocyte cell body
B: fenestrations
C: foot processes of podocytes
D: filtration slits
E: cytoplasmic extensions of podocytes
Label A-D

A: clavicle
B: Cardiophrenic angle
C: costophrenic angle
D: hila of lungs
Label A and B

A: cortex
B: medulla
Label A - D

A: thoracic aorta
B: posterior intercostal artery and vein
C: interior intercostal artery and vein
D: internal thoracic artery and vein
E: azygos vein
What condition is this?

Oedema
Label A-C

A: hilum - where the 2 pleural layers fuse
B: visceral pleura - attached to thoracic wall
C: parietal pleura - covers lungs
Label A and B, and what they’re innervated by. What is C?
What is between A and B, and what is its function?

A: Visceral pleura, innervated by sympathetic nerves, covers external lung surface
B: parietal pleura, innervated by intercostal nerves T2-12
C: Phrenic nerves C3-5
Pleural fluid, reduces friction so tissue doesn’t wear, and creates surface tension. PF produced by parietal pleura.
What is FS?

Fatty streak (foamy macrophages, few lymphocytes and rare SM cells) in sub intimal layer.
How would you describe the following two Xrays?

A: underpenetrated
B: overpenetrated
Label A and B. What do they secrete?

A: adrenal cortex, secretes cortisol
B: adrenal medulla, secretes adrenaline
What are A,B, and C?

A: fibrous pericardium
B: parietal pericardium
C: visceral pericardium
What can you see in leads II and III?

S-T elevation
Label A-E
What part of the X-ray examination is this?

A: R. main bronchus
B: trachea
C: aorta
D: L. main bronchus
E: carina
Airways
What does this CXR show and why?
What causes this condition? Give values.
What symptoms may this condition cause?

Pulmonary oedema - shows peri-hilar oedema (batwing) and kerley B-lines (fluid drained away by lymphatics so can see horizonal lines through lungs but hard to see)
Pulmonary venous hypertension (>25mmHg venous pulmonary pressure)
Respiratory distress and crackles, orthopnea (SoB when lying flat)
Label A, B and C

A: costophrenic recess
B: costophrenic angle
C: cardiophrenic angle
What is this muscle?

Skeletal
What are A-C?

A: Left Coronary Artery
B: L. circumflex
C: Anterior interventricular (LAD)
What kind of cell is this?

Reticulocyte
What kind of cells are in A and B and what is the difference between them?

Blood cells.
A: in bone marrow, thicker b/c nuclei present, more viscous
B: in blood, more fluid
What are 6, 9 and 10?

- Internal thoracic artery
- Thyrocervical trunk
- Costocervical trunk
Label 1-4

1: frontal sinus
2: ethmoid sinus
3: sphenoidal sinus
4: maxillary sinus
Are these Xrays rotated?

A is, B isn’t
Spinous processes should be straight and lie mid-way between medial head of clavicles.
With A : clavicles asymmetrical, no clear spinous process in middle
This tumour is trying to invade a tissue in the submucosa of the airway. What kind of tissue is the arrow indicating?

Hyaline cartilage
Label A-D

A: capsule (CT)
B: cortex
C: medullary pyramids
D: ureter
Label A-C

A: small saphenous vein
B: great saphernous vein
C: dorsal venous arch
What is A?

Azygos vein
Label A-D

A: brachial plexus
B: Phrenic nerve
C: Internal thoracic (mammary) artery
D: External intercostals
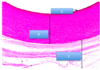
What are the 2 changes to look out for in asthma, labelled here?

Increase in smooth muscle mass (2)
Fibrosis underlying epithlial BM (1)
Label A-D

A: Medulla
B: Cortex (lymphocytes!)
C: Fibrous capsule
D: Trabeculae
Label A-D

A: R lymphatic trunk
B: Venous angle
C: Thoracic duct
D: cisterna chyli
Label the lymph nodes A-E

A: preauricular
B: submental
C: submandibular
D: superficial cervical
E: deep cervical
Label A-C

A: cisterna chyli
B: pre-aortic LN
C: lumbar LN
Label A and B

A: Splenic artery
B: Spleen
What is wrong with this lady?

Lymphodema in L arm as result of masectomy. Remove axillary lymph nodes = increases chance of lymphodema but reduces chance of metastasis.
Label A-F

A: medulla
B: cortex
C: hilum
D: renal papilla (where medullary pyramids empty urine into minor calyx)
E: interlobar arteries
F: interlobular arteries
What are the structures indicated by the arrows and stars in the kidney?

Arrows: renal corpuscles (glomerulus + Bowman’s capsule)
Stars: medullary rays composed of collecting ducts
The upper half of this photomicrograph is renal cortex, and the lower half renal medulla. What is A and the arrows?

A: arcuate vessel
Arrows: medullary rays
What renal structure is this in the centre, and what part of it are the arrows pointing to?
What are the whitish shructures A and B?

Bowman’s capsule. Parietal layer indicated by arrows is made of simple squamous endothelium
A: distal convoluted tubule
B: proximal convoluted tubule (bigger b/c more absorption going on)
What are the cell processes indicated by A?
What is indicated by B?
What cells are inside B?

A: podocyte foot
B: basement membrane
C: endothelial cells are inside BM
What abnormality does the patient’s glomerulus show by light microscopy?
What abnormality is seen on EM?
What is the diagnosis?

Diffuse thickening of capillary walls, may be due to expansion of BM or increased mesangial matrix.
Electron dense deposits on epithelial aspect of BM = antigen-antibody complexes
Membraneous glomerulonephritis (associated wtih hep B, malaria, tumours)
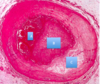
What are the renal tubules indicated by the arrows lined by cells (luminal surfaces stained black for alkaline phosphatase)?
What are the unstained tubules indicated by the arrowheads?
Why are lysosomes in the arrowed tubules?
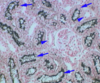
Stained: PCT
Unstained: DCT
Break down large proteins and carbs that are endocytosed from provisional urine by proximal tubules
What are A-C in the kidney?

A: vasa recta
B: thin limb of LOH
C: collecting duct
A 55yo woman presented with a 2 week history of painless haematuria. Imaging investigations showed a renal mass. A L nephrectomy was performed.
What macroscopic abnormality do you see?
What type of cells make up the lesion?
What is the diagnosis?
What haematological abnormalities may this pt have as a result of this lesion?

Yellow-brown mass in upper pole of kidney with central area of necrosis
Clear cells make up lesion - arise from tubular cells and clear due to their high content of glycogen and lipids
Renal cell carcinoma (clear cell carcinoma most common type)
Haematuria may cause iron deficiency anaemia. This tumour may produce EPO, so the pt may develop polycythaemia.
Identify the layers of the ureter wall A-D.

A: transitional epithelium
B: lamina propria or submucosa
C: muscularis
D: adventitia (not serosa because the ureter is not covered by mesothelium)
Ureter
What is another name for this type of epithelium?
Where else is it found?
Name 2 properties of this epithelium that make it most suited for its location.
From where does this epithelium derive its nutrients?

Transitional epithelium (umbrella cells)
Kidney calyces, renal pelvis, bladder, urethra
Allows distension and forms impervious barrier to urine
Underlying CT (like all epithlial linings)
What can you see in this CXR?

Consolidation of L upper lobe, classical for S. pneumonae - pneumonia
What can you see in these images of the lung and sputum gram stain?
L: lobar consolidation on L
R: lots of G+ cocci and pus
What can you see on these CXRs?

L: pleural effusion and patchy consolidation on L, fluid would have to be aspirated/drained
R: 2 huge abceses full of fluid (prob pus) on R, would need chest drain/surgical
What can you see on this CXR? What would you diagnose the patient with?

Ghon focus: on bottom R (10 lesion stuck to pleura, caused by TB (mycobacterium bacilli), small area of granulomatous infection only detectable on CXR if it calcifies/grows substantially.
Gohn complex: when the GF involves infection of adjacent lymphatics and hilar lymph nodes.

What is this condition?

Pseudomembrane - diptheria