Vascular Flashcards
(101 cards)
Post-phlebitic limb: chronic venous insuficiency
Examination
(Inspection, palpation, completion, special test)
Inspection
- Venous Infufficiency (HAS LEGS)
- Haemosiderosis; damages capillaries leak blood -> read brown patches
- Atrophie blanch
- Swelling, ankle (chronic v insuff/DVT/HF)
- Lipodermatosclerosis; inflammation of subcutaneous fat-> woody hard skin
- Eczema, venous
- Gaiter ulcers
- Stars, venous
- Varicose veins: Superficial venous dilation and tortuosity.
- Present as collaterals bypassing the obstruction
Palpation: pitting oedema
Completion
- Perthe’s test;
- Tests for deep venous occlusion
- High tourniquet around pts. leg + walking for 5min
- Deep obstruction → swelling and pain
- Abdominal exam + PR
- Pelvic exam in women
Post-phlebitic limb: chronic venous insuficiency
History
Hx
- Previous DVT; Orthopaedic surgery/Complicated obstetric
- Venous Claudication: “Bursting” pain in the leg after exercise, Relieved by rest and elevation of limb (cf. arterial)
Post-phlebitic limb: chronic venous insuficiency
causes
Reflux following DVT: 90%
Obstruction following DVT: 10%
Post-phlebitic limb: chronic venous insuficiency
venous gangerne
(What? 3 phase)
- Rare complication of DVT in the iliofemoral segment
- 3 phases
- Phlegmasia alba dolens: white leg
- Phlegmasia cerulea dolens: blue leg
- Gangrene 2O to acute ischaemia
Post-phlebitic limb: chronic venous insuficiency
Lipodermatosclerosis (viva)
Lipodermatosclerosis
- Panniculitis
- Venous HTN → extravasation of fibrin and red cells
- Poor tissue oxygenation → ulceration and fat necrosis
- Inverted champagne bottle appearance
- Chronic inflam → fibrosis → distal shrinkage
- Venous obstruction → proximal leg swelling
Post-phlebitic limb: chronic venous insuficiency
Ix of Deep Venous Disease
Ix of Deep Venous Disease
- Duplex: reflux and occlusion
- Venography
- Ascending: patency and perforator incompetence
- Descending: reflux
- Ambulatory venous pressures
Post-phlebitic limb: chronic venous insuficiency
Surgical options (reflu/obstruction)
Surgical Options
Reflux
- Trahere Transplantation
- Transplant segment of axillary vein c¯ valve into deep venous system of leg
- Wrap c¯ PTFE cuff
- Kistner Operation
- Valvuloplasty of damaged valves
Obstruction
- Palma operation
- Use contralateral GSV and anastomose to femoral vein to bypass iliofemoral obstruction
Venous
Examination
(inspect, palpate, ausculation, other)
Inspect;
- Scars; esp in groin creases
- skin colour changes
- Venous Infufficiency (HAS LEGS)
- Haemosiderosis; damages capillaries leak blood -> read brown patches
- Atrophie blanch
- Swelling, ankle (chronic v insuff/DVT/HF)
- Lipodermatosclerosis; inflammation of subcutaneous fat-> woody hard skin
- Eczema, venous
- Gaiter ulcers
- Stars, venous
- Varicose veins: Superficial venous dilation and tortuosity
- Distribution;
- medial and above the knee; great saphenous
- Posterior and below the knee; short saphenous
- Few varicosities and prominent skin changes; calf perforators
- Distribution;
- ?Inverted champagne bottle leg
Palpate
- Pitting oedema; if present establish how far oedema extends; also check JVP if oedema is found
- Palpate varicosities
- Tenderness/hardness: thrombophlebitis
- Induration: thrombosis
- Saphena varix @ SFJ
- Two finger breaths below and lateral to pubic tubercle
- Bluish tinge, disappears on lying flat
- May have cough impulse (Cruveihier’s Sign)
- Calf tenderness (DVT)
Percussion (wave of varicosities; tap distally and feel impulse proximally (normal) and tap proximally and feel impulse distally (incompetent valves))
- Tap test (Chevrier’s Test)
- Tap proximally and feel for impulse distally
- Distal pulses: PTA, DPA
Auscultation ; bruit over varicosity; AVM
Other
- Trendelenburg (/tourniquet) test if varicosities present; determines the position of venous regurgitation of varicosities in leg.
- Elevate limb to 15* and note rate of venous emptying
- Position patient supine, Lift pt leg as high as comfortable and milk leg to empty the veins. While elevated place tourniquet/press thumb over saphenofemoral junction (2-3cm below and 2-3cm lateral to pubic tubercle) ask pt to stand while pressure is maintained.
- Controlled: incompetence above tourniquet. Release tourniquet to confirm filling
- Uncontrolled: incompetence below tourniquet e.g. SPJ or calf perforators. Repeat test with tourniquet just below knee
- Examine the abdomen and perform a PR
- Pelvis examination in females
- Pulses (arterial)
- Doppler; Place probe @ SFJ/SPJ and squeeze calf. Normally hear only half second whoosh when pressure released. Long whoosh suggests valve incompetence.
Varicose veins
presentation
presentation: Abnormal, Tortuous, dilated veins of the superficial venous system. clearly in the distribution of the LSV in the medial side of the thigh and calve. These can be primary: which 99% are, which replies a failure of the valves and reflux down the superficial venous system. They can be secondary; as a result of blockage in the deep viens and increased pressure on the venous system higher up.
Varicose veins
symptoms and complications
Symptoms:
- Cosmetic defect
- Pain, cramping, heaviness
- Tingling
- Bleeding: may be severe
- Swelling
Complications;
- Swelling and oedema
- Thrombophlebitis
- Bleeding
- Varicose eczema
- Haemosidering deposition-> lipodermatosclerosis (woody, champagne bottle)-> venous ulceration
Varicose veins Investigations
Duplex US
- Indications
- Previous Hx of DVT
- Signs of chronic venous insufficiencyl Suggests deep venous disease for which the varicosity may be the collateral.
- Recurrent varicose veins
- Difficulty in deciding whether GSV or SSV is incompetent
Preparation for Surgery
- FBC, U+E, clotting, G+S
- CXR
- ECG
Varicose veins classifications
CEAP Classification, Classification of Chronic Venous Disease
- Clinical signs (1-6 + sympto or asympto)
- Etiology
- Anatomy
- Pathophysiology
Varicose veins management
Conservative
- Lose wt. and regular exercise
- Avoid prolonged standing
- Class II graduated Compression Stockings; 18-24mmHg
- Skin care: emollients
Minimally Invasive Therapies (Indications; Small below knee varicosities not involving GSV or SSV)
- Techniques
- Local or GA
- Injection sclerotherapy: 1% Na tetradecyl sulphate
- Endovenous laser or radiofrequency ablation
- Post-Operatively
- Compression bandage for 24hrs
- Compression stockings for 1mo
Surgery (Indications; SFJ incompetence//Major perforator incompetence// Symptomatic: ulceration, skin changes, pain)
- Procedures
- Trendelenberg: saphenofemoral ligation
- SSV ligation: in the popliteal fossa
- LSV stripping: no longer performed due to potential for saphenous nerve damage.
- Multiple Avulsions
- Cockett’s Operation: perforator ligation
- SEPS: Subfascial Endoscopic Perforator Surgery
- Post-op
- Bandage tightly and elevate for 24h
- D/C c¯ compression stockings and told to walk daily.
- Complications:
- Early
- Haematoma: esp. groin
- Wound sepsis
- Nerve damage: e.g. long saphenous
- Late
- Superficial thrombophlebitis
- DVT
- Recurrence: 10% @ 5yrs
Varicose veins
pathophysiology
- One-way flow from sup → deep maintained by valves
- Valve failure → ↑ pressure in sup veins → varicosity
- Fibrous tissue invades tunica intima and media, breaking up the SM
- Prevents maintenance of vascular tone → dilatation
- 3 main sites where valve incompetence occurs
- SFJ: 3cm below and 3cm lateral to pubic tubercle
- SPJ: popliteal fossa
- Perforators: draining GSV
- Chronic venous insufficiency is distinct and results from incompetency in the deep system itself.
- May co-exist c¯ varicose veins
Varicose veins
causes
- Primary / Idiopathic: 95%
- Prolonged standing
- Pregnancy
- Obesity
- OCP
- Secondary: 5%
- Valve destruction: DVT, thrombophlebitis
- Obstruction: pelvic mass, DVT
- AVM
- Syndromes
- Klippel-Trenaunay-Weber
- Abnormality of the deep venous system
- Varicose veins
- Port wine stain
- Bony and soft tissue hypertrophy of the limbs
- Parkes-Weber Syndrome
- Multiple AVMs c¯ limb hypertrophy
- AVMs can → high-output HF
- Klippel-Trenaunay-Weber
Lymphoedema
Examination
(inspect, palpate, complete)
Inspection
- Gross leg swelling
- Bilateral or unilateral
- Thick, indurated skin
- Lichenification
- Yellow nail discoloration
Palpation
- Initially: pitting
- Later: non-pitting
- Palpate for inguinal nodes
Completion
- Exclude RHF: ↑ JVP, Hepatomegaly
- Take a Hx: esp. re hereditary conditions
Lymphoedema
vival
DDiagnosis; bilateral and unilateral limb swelling
Bilateral
- ↑ Venous Pressure
- RHF
- Venous insufficiency
- Drugs: e.g. nifedipine
- ↓ Oncotic Pressure
- Nephrotic syndrome
- Hepatic failure
- Protein losing enteropathy
- Lymphoedema
- Myxoedema; Hyper- / hypo-thyroidism
Unilateral
- Venous insufficiency
- DVT
- Infection or inflammation
- Lymphoedema
Lymphodema
define
Pimary and secondary causes
Define: Collection of interstitial fluid due to blockage or absence of lymphatics.
Primary; Congenital absence of lymphatics. May or may not be familial. Presentation:
- Congenital: evident from birth.
- Praecox: after birth but < 35yrs
- Tarda>35 yrs
- Milroy’s Syndrome: 2% of primary lymphoedema. Familial AD subtype of congenital lymphoedema F>M
Secondary: FIIT
- Fibrosis: e.g. post-radiotherapy
- Infiltration
- Ca: prostate, lymphoma
- Filariasis: Wuchereria bancrofti
- Infection: TB
- Trauma: block dissection of lymphatics
Lymphoedema
Viva; Management
(conservative, physio, surgical)
Conservative
- Skin care
- Grade 3 compression stockings
- Treat or prevent cellulitis
Physio
- Raise leg as much as possible
Surgical
- Debulking operation
- Bypass procedures
Peripheral Ulcer Examination
Inspect, palpate, complete
Inspection: BEDS
- 3s: Site, Size, Shape
- Base:
- Granulation tissue
- Slough
- Floor: bone, tendon, fascia
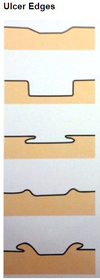
- Edge:
- Sloping: healing – usually venous
- Punched-out: ischaemic or neuropathic
- Undermined: pressure necrosis or TB
- Rolled: BCC
- Everted: SCC
- Discharge: Serous, Purulent, Sanguinous
- Surroundings: Cellulitis, Excoriations, Sensate, LNs
Palpation
- Limb pulses
- Sensation around the ulcer
Completion
- Examine contralateral side
- Distal neurovascular examination
- ABPI: must be >0.8 for compression bandaging
Causes of PEripheral ulcer
Causes;
Venous: 75% + Arterial: 2% + Mixed arteriovenous: 15% + Neuropathic
Other: Pressure, Vasculitis: e.g. PAN, Malignancy: SCC, Marjolin’s, Systemic: pyoderma gangrenosum
Venous ulcer
Findings on Examination
(inspect/palpate)
Inspection Site: medial malleolus, Size: variable, can be v. large, Base: Shallow and Pink granulation tissue, Edge: sloping edge, Discharge: seropurulent Surroundings: Signs of chronic venous insufficiency: HAS LEGS and Varicose veins
Palpation Painless, Warm surroundings, Sensate
Venous ulcer
viva causes
Valvular disease Varicose veins Deep vein reflux: e.g. post DVT Outflow obstruction (Often post DVT) Muscle pump failure Stroke Neuromuscular disease
Venous ulcer
Investigations
ABPI if possible
Duplex ultrasonography
Biopsy may be necessary: esp. if persistent ulcer
Look for malignant change: Marjolin’s ulcer