10/16- Appendix and Peritoneum, Pathology Flashcards
(62 cards)
>95% of biliary tract disease is attributable to ____
>95% of biliary tract disease is attributable to cholelithiasis
- > 20M Americans in the US have gallstones
- Cholecystectomy done 600,000/yr (one of most common abdominal operations)
Describe the anatomy of the gallbladder

Describe the histology of the gallbladder (layers)
- Mucosa
- No discrete muscularis mucosae/submucosa
- Fibromuscularis layer
- Subserosal fat with vessels
- Serosa
- Except no serosa on hepatic bed

Characteristics of gallstones
- Prevalence in developed countries
- More silent or symptomatic
- Percentage undergoing surgery
- Risks/associations
- Common stone composition
- Prevalence in developed countries: 10-20% of adults
- More silent (>80%)
- Percentage undergoing surgery: > 50%
- Gallbladder cancer in long-standing cholecystitis with gallstones
- Cholesteral stones are common (80%)
- > 50% crystalline cholesterol monohydrate
What is seen here?

Gallstones (?)
What are the different types/presentations of cholecystitis?
Acute
- Acalculous (without stones)
- Calculous (with stones)
Chronic
- Almost always in the setting of a gallstone
What is seen here?

Acute cholecystitis
What is seen here?

Acute cholecystitis
What is seen here?
Chronic cholecystitis
Characteristics of gallbladder carcinoma
- Common or Rare
- Age of onset
- Gender
- Most common type
- Associated factors
Intestinal metaplasia -> dysplasia
- Relatively uncommon
- most > 60 yo (average 72 yrs)
- 75% women
- Mostly adenocarcinoma (90%)
- Associated factors: gallstones (2/3)
What is seen here?

Gallbladder carcinoma
What is seen here?

Gallbladder carcinoma
What is seen here?

Gallbladder carcinoma
What pathology can occur with the appendix?
- Acute and chronic inflammation
- Tumors
Describe anatomy of the appendix- what is it?
- Length
- Diameter
- Layers
- Long, narrow and worm-shaped tube
- Normal true diverticulum of the cecum
- 1-9” long; 3” in diameter on average
- Mucosa, submucosa, muscularis propria(?) and serosa
- Mucosa: abundant lymphoid tissue especially in young people
Layers of appendix?
- Mucosa with crypts of Lieberkuhn
- Submucosa
- Circular muscle
- Longitudinal muscle
- Serosa (visceral peritoneum
- Mesoappendix

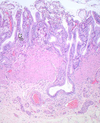
What is seen here?

Appendix
- Mucosa
- Submucosa
- Muscularis mucosa
- Serosa

What is the function of the appendix?
- Uncertain
- Mucosal immunity
- B cell lymphocyts from appendix migrate and populate distant sites of gastrointestinal lamina propria and evolve into functional IgA secreting plasma cells
Characteristics of acute appendicitis:
- Age
- Lifetime risk
- Gender
- DDx includes
- Most in adolescents and young adults
- Lifetime risk = 7%
- More in males
- Confused with other intra-abdominal or pelvic pathologies
How does acute appendicitis present?
- Periumbilical pain, RLQ pain
- N/V, low-grade fever
- Mildly elevated WBC
- Classic physical finding: McBurney’s sign
- On spinoumbilical line
Diagnosis of acute appendicitis in young children and elderly is problematic (atypical clinical presentations)

What are complications of acute appendicitis?
- Perforation
- Pyelophlebitis
- Portal venous thrombosis
- Liver abscess
- Bacteremia
What is seen here?

Removed appendix (acute appendicitis?)
Describe the pathology of acute appendicitis
- Early
- Diagnosis
- Severe
Early phase:
- Congestion of subserosal vessels with
- Modest perivascular neutrophilic infiltrate of all layers of the wall
Diagnosis:
- Neutrophilic infiltration of the muscularis propria
More severe cases:
- Prominent neutrophilic exudate generates a serosal fibrinopurulent reaction
What is seen here?

Appendicitis
- Focal ulceration of mucosa
- Collection of neutrophils


























