8 - Disorders of the Knee Flashcards
What are the best ways to x-ray image the knee?

When do femoral shaft injuries occur?
- High velocity trauma e.g RTA
- Child abuse
- Osteoporotic or bone lesions can lead to fractures with low velocity e.g falling over from standing

Who is at risk of getting knee disorders?
- Elderly
- Obese people
- Athletes
What is the danger of femoral shaft injuries?
- Hypovolaemic shock due to blood loss of around 1-1//5 litres in closed fracture, can be double this in open fracture
- Fix surgically

How does a femoral shaft get deformed after fracture and why?
- Proximal part usually abducted due to glut med and min on greater trochanter
- Proximal flexed due to iliopsoas on lesser trochanter
- Distal adducted into varus deformity due to adductor muscles and extended due to gastrocnemius on posterior femur

What is a distal femoral fracture, who is at risk and what is the major risk with this type of fracture?
- Young people in high energy sporting injury or old person with osteoporotic bone and a fall
- Popliteal artery can become involved so have to assess status of limb before and after reduction of fracture
https://chestofbooks.com/health/anatomy/Human-Body-Construction/Fractures-Of-The-Femur-Continued.html

What do tibial plateau fractures look like?
- Due to high energy injuries of axial loading with valgus or varus angulation of knee
- Uni/Bicondylar (mainly lateral tibial condyle)
- Articular cartilage always damage so fracture fragments have to be removed but almost always get OA after surgery
- These fractures associated with ACL injuries and meninscal tears

What are the causes of a patella fracture, what are the two types and how are they treated?
- Direct impact injury (e.g dashboard) or eccentric contraction of quadriceps (e.g skiing)

Displaced:
- Reduce and fix
Undisplaced:
- Splint and protect e.g crutches
How can you tell when examining a patient that they may have a patellar fracture?
- Palpable defect in patella
- Haemarthrosis in joint
- Extensor mechanism may be disrupted if fracture splits patella distal to insertion of quadriceps tendon (displaced fracture)

Why may a patient appear to have a patellar fracture but they haven’t had any trauma?
- Bipartite patella
- Failure of union via ossification so fibrocartilage remains

What is the difference between patella dislocaiton and subluxation?
- Dislocation is when patella is completely displaced from normal alignment
- Subluxation is partial displacement

What is the most common way for the patella to dislocate, why, and how does the anatomy of the knee try to avoid this?
- Laterally
- Q angle between pull of quad tendon and patellar ligament means most likely to go laterally
- Usually VMO contraction stabilises patella in trochlear groove and controls tracking of patella

What movement is most likely to cause patellar dislocation and who is predisposed to these injuries?
- Twisting injury in slight flexion or direct blow to knee
- Mainly sporty teenagers with internal rotation of femur on planted foot whilst flexing knee
Who?
- Generalised ligamentous laxity
- Weakness of quad muscles, e.g VMO
- Shallosw trochlear groove with flat lateral lip
- Long patellar ligament
- Previous dislocations
How do you treat a patella dislocation?
- Extending knee and manually reducing patella
- Immobilisation during healing
- Physiotherapy to strengthen VMO

When do meniscal tears occur and what do they look like on MRI?
- Sudden twisting motion of weight bearing knee in high degree of flexion
- May be some knee joint effusion too due to fluid and fluid in area of tear (white)

What are the two types of meniscal tear and how are meniscal tears treated?
- Acute usually surgical meniscetomy or meniscal repair
- Degenerative usually rehabilitation and conservative as surgical not long prognosis

What will the patient normally present with with a meniscal tear?
- Intermittent pain localised to joint line
- Knee clicking, catching and locking
- Giving way sensation
- Swelling may be delayed symptom due to reactive effusion

What does locking of the knee mean when a patient describes it?
Inability to full extend knee due to intra-articular foreign body

What things affect the knee stability?
- Static: bones and ligaments
- Dynamic: muscles and tendons

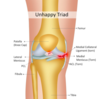
What is the unhappy triad?
- Three tears due to a strong force applied to the lateral aspect of the knee
- Medial meniscus is adherent to medial collateral ligament which is why it tears too
What is the role of the collateral ligaments and how are they injured?
- Control lateral movement of knee joint and brace against unusual angulation
- Also, work with PCL to prevent excessive posterior motion of tibia on femur.
- Injured due to acute varus or valgus angulation of knee

What will patients present with when they have a collateral ligament injury?
- Pain and swelling of knee immediately
- Joint unstable and patient complains of giving way or not supporting body weight
- Brace and rehab or surgery with unhappy triad

What collateral ligament breaks with each strain?
- Valgus: medial at risk (more common)
- Varus: lateral at risk
- LCL break will cause more knee instability as shallower socket for femoral condyle on lateral side

What does the ACL normally do and how is it torn?
- Controls rotational stability of the knee
- More common tear than PCL
- Quick deceleration, hyperextension or rotational injury (sudden change in direction) can cause tear
- Usually non contact injury
- Can be torn by large force to back of knee in slight flexion

What does an ACL tear normally present as and how is it fixed?
- Popping sensation with immediate swelling
- Instability of knee due to tibia sliding anteriorly ‘giving way’
Treat:
- Low functional demand on knee can use musculature to stabilise joint
- Sportsman need surgical reconstruction

How does PCL tear occur?
- Dashboard injury as knee is flexed and large force applied to upper tibia displacing it posteriorly
- Person falling on flexed knee with ankle plantarflexed
- Tackle with knee flexed
- Severe hyperextension can avulse PCL from it’s insertion

What tests can be done to check the stability of the cruciate ligaments?
- Lachman’s Test (ACL)
- Anterior and Posterior Drawer tests

How do you dislocate the knee, what are the complications and how do you treat it?
- Uncommon and due to high energy as have to rupture 3 out of 4 ligaments
- Popliteal artery injury as tethered proximally. Can lead to haematoma, be crushed or traction injury leading to thrombotic occlusion
- Reduce and stabilise and then test vasculature with MRA

What are some of the causes of swelling around the knee?
- Bony: Osgood-Schlatter’s
- Soft tissue: localised popliteal lymph node or artery. generalised lymphoedema
- Fluid: effusion in joint or soft tissue haematoma outside

What are the two main types of knee effusions?
Acute: <6 hours after injury due to haemarthrosis
Delayed: >6hours after injury due to reactive synovitis, inflammation of synovium so more synovial fluid
NEVER NORMAL

What are the two types of acute knee effusion and what do they indicate?
- Haemoarthrosis: blood in joint
- Lipo-haemarthrosis: blood and fat in joint due to release from bone marrow

What is pre-patellar bursitis?
- Housmaid’s knee
- Knee pain and swelling with redness overlying inflammed bursa
- Patient cannot walk or kneel due to pain
- History of repetitive trauma or may be history of blunt trauma to knee up to 10 days after incident

What is infrapatellar bursistis?
- Clergyman’s knee
- Mostly affects superficial infrapatellar bursa
- Repetitive microtraume by activities involving kneeling

What is suprapatellar bursitis?
- This bursa is extension of synovial cavity so knee effusion usualy presents with swelling in this pouch
- Shows got a swelling in knee joint

What is semimembranosus bursitis?
- Indirect consequence of swelling in knee joint
- Attached to posterior capsule of knee joint beneath deep fascia of popliteal fascia
- If effusion in knee joint, fluid can force way out of small opening into semimembranosus bursa
- Popliteal cyst or Baker’s cyst

What is Osgood-Schlatter’s Disease (OSD)?
- Inflammation of apophysis (insertion) of the patellar ligament onto tibial tuberosity
- In sporty teenagers and can cause localised pain and swelling
- Bilateral 20-30% cases
- Intense knee pain during running, jumping, squatting, climbing stairs and kneeling
- Resolves with rest and ice. Pain and swelling resolve at age of skeletal maturity as apophysis fuses but bony prominence remains

What are the typical symptoms of knee OA?
- Knee pain, stiffness and swelling
- Knee pain comes and goes, precipitated by activities, pain and stifness after prolonged inactivity
- Valgus, varus or fixed flexion deformity
- Crepitus
- Effusion
- Buckling knee (quad muscle weakness and instability of knee)
- Uni, bi or tricompartmental

What is the initial treatment for knee OA?
- Strengthen vastus medialis muscle to reduce instability
- Weight loss
- Analgesia
- Activity modification
- Finally total knee replacement

What is the best way to image for osteoarthritis of the knee?
Weightbearing so can see if bicompartmental etc

What is septic arthritis?
- Most common knee, hip, shoulder, ankle wrists
- Most common is Staph aureus. Can be staph.epidermidis, neisseria gonnorhoeae, step.viridans, strep,pneumoniae and Group B streptococci
- Bacteria damage articular cartilage directly, e.g proteases from Staph.aureus, or stimulate neutrophils to hydrolyside collagen and proteoglycans

What do patients with septic arthritis usually present with?
- Symptom triad: Fever, Pain, Reduced range of motion developing over few days or weeks
- Erythema, swelling, warmth, tenderness, limited range of movement
- In prosthetics not much swelling or symptoms but may find draining sinus from underlying infected joint
What should you do if you suspect septic arthritis?
- Immediate aspiration of joint and aspiratie sent for urgent culture
- Surgical washout and antibiotics
(most people have decreased range of motion and chronic pain if resolved and don’t die)
