MSCT Week 5: Papulosquamous Skin Eruptions Flashcards
Papulo means in papulosquamous eruptions
Plaque - raised skin lesion with epidermal component
Squamous in papulosquamous means
scale or excess shedding of keratinocytes
Pathology?


Pathology?


Hyperkeratosis is?
Thickened Stratum Corneum
Parakeratosis is?
Presence of keratinocytic nuclei in the stratum corneum
Acanthosis is?
Thickened spinous layer also known as epidermal hyperplasia
Acanthosis AKA?
Epidermal Hyperplasia
Pathology?


Descriptions

Pathology?

- Acanthosis
- Hyperkeratosis
- Parakeratosis
Pathology?

Acanthosis
Hyperkeratosis
cant see Parakeratosis
Pathology?

- Hyperkeratosis
- Parakeratosis
- Neutrophils in the stratum corneum
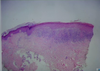
Pathology?

Hyperkeratosis
Parakeratosis
acanthosis might be hard to see from this magnification
neutrophils in the stratum corneum
What is Psoriasis?
A chronic, inflammatory skin condition
Psoriasis prevalence?
- 2% of the US population
- can be seen at any age, peaks in diagnosis in early 20s and middle age
Psoriasis Risk Factors
Strong genetic component (1/3 have affected 1st degree family)
Psoriasis Characteristics
2 listed
- Waxes & Wanes but has a chronic tendency
- May or may not be itchy
Psoriasis Characteristics Overview

Psoriasis Age of Onset
can be seen at any age, peaks in diagnosis in early 20s and middle age
Psoriasis Morphologies
8 listed
Plaque
Guttate
Inverse/Flexural
Generalized/Erythrodermic
Pustular
Acral/Palmoplantar
Auspitz Sign = pinpoint bleeding in dermis when scale removed
Clinical pearl: Nail Pitting

Guttate Psoriasis
Having drops or droplike markings
Inverse/Flexural Psoriasis appears where on the body?
in the skin folds like arm pits
Psoriasis type?

Plaque
Psoriasis type?

Inverse/Flexural
Psoriasis type?

Generalized/Erythrodermic
Psoriasis type?

Guttate
Psoriasis type?
Pustular
Psoriasis type?

Acral/Palmoplantar
Common locations of psoriasis

Identify


Identify


Topical Treatments for Psoriasis
5 listed

Systemic Treatments for Psoriasis

Psoriatic Arthritis and other comorbidities

Pathology?

Atopic Dermatitis
- Spongiosis (desmosomal attachments visible between keratinocytes)
- eosinophils in the bottom left
- langerhans cells
Atopic Dermatitis is most commonly found where on the body?

Identify


Histology for Atopic Dermatitis

Pathology?

- Atopic Dermatitis
- spongiosis

What Percentage of children with atopic dermatitis will have or develop another atopic condition?

50-80%

Pillars of treatment: Atopic Dermatitis
4 listed
- issue with skin barrier so prevent infection or treat with antibiotics, irritants or allergens Topical antibiotics
- addressing the itch-rash cycle (oral antihistamines)
- Anti-inflammation (topical cortical steroids (rarely systemics)

Question 1

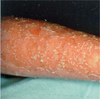
Allergic Contact Dermatitis
Allergic Contact Dermatitis (ACD) clinical description

Question 2

reddish polygonal pruritic bumps on the wrist
Identify


Pathology
- hypergranulosis
- band of lymphocytes at the dermal-epidermal junction (lykinoid infiltrate)
- sawtooth of Rete Ridges
- Lichen Planus