Basic Bone Biology - what is bone made of?
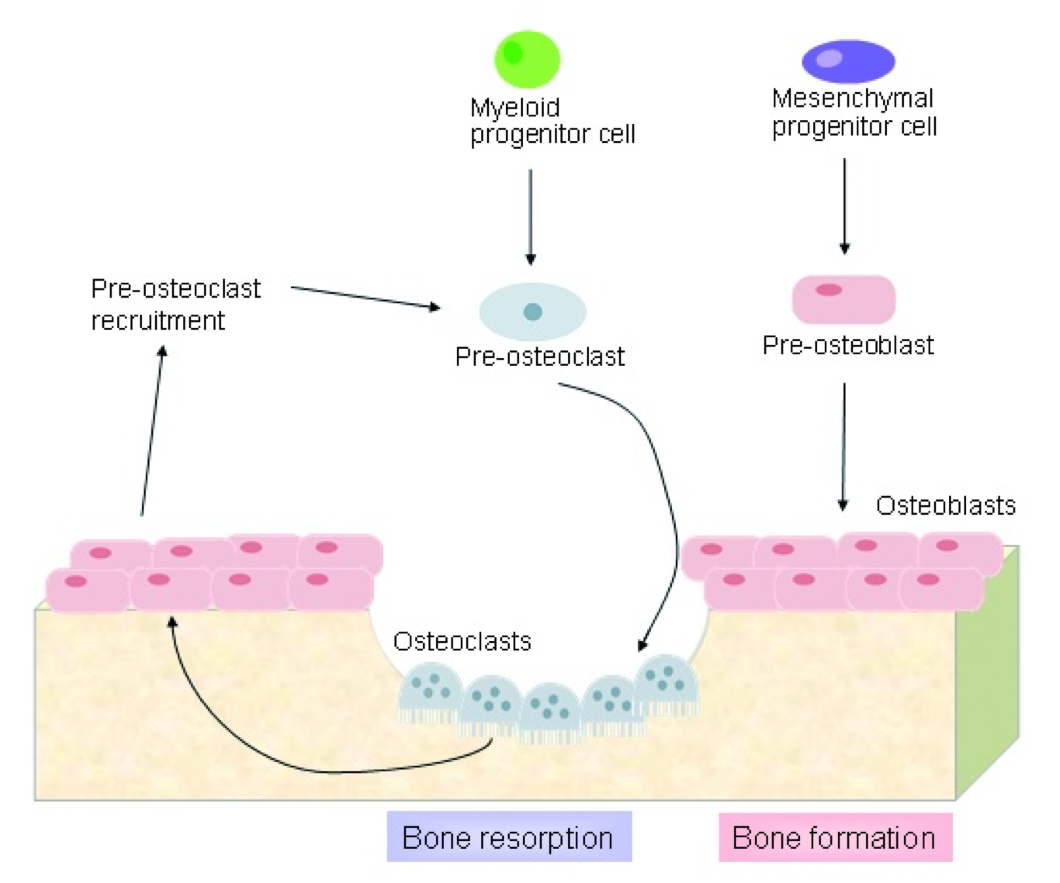
Osteoblasts – makes bone
Osteoclasts – breaks down bones
Bone remodelling
cycles
Depends at different rates depending on age of individual and clinical circumstances
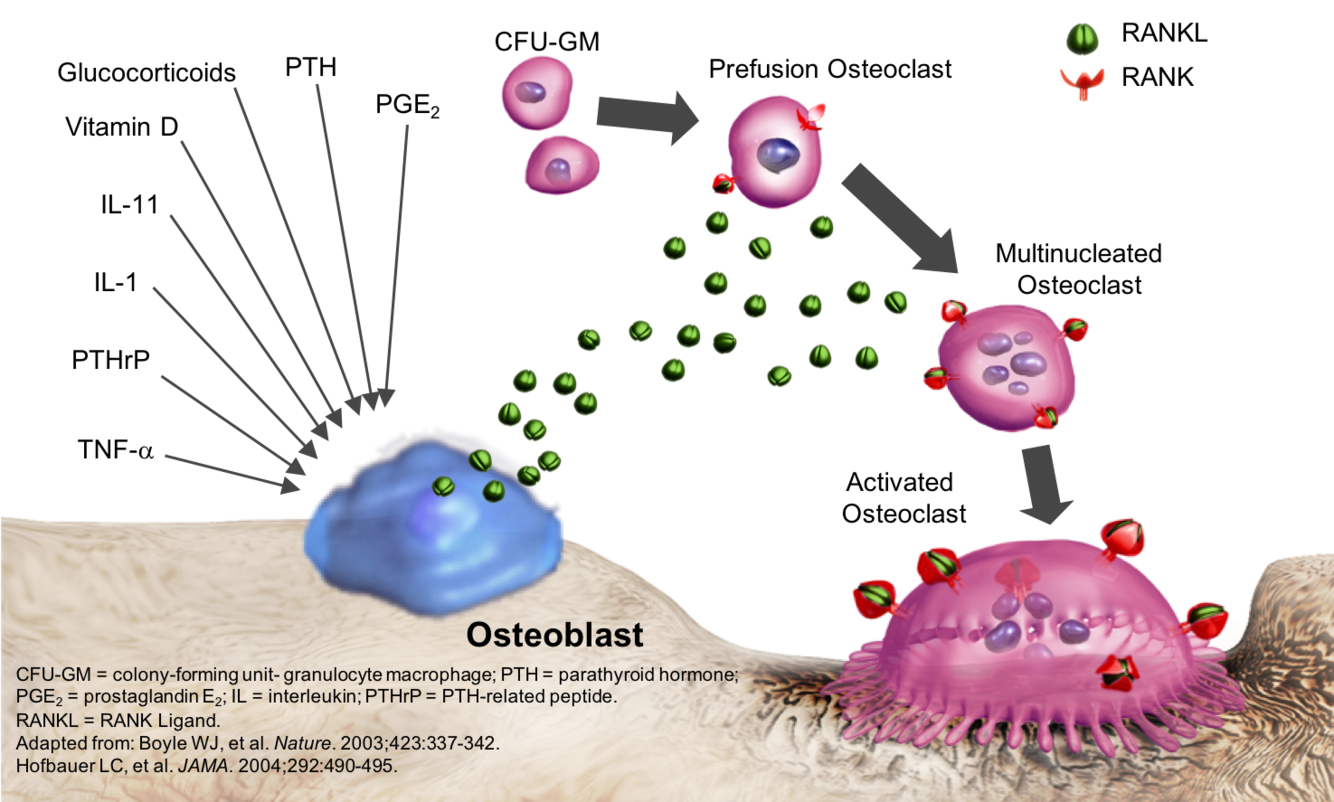
Many Factors Stimulate Osteoblast Expression of RANK Ligand such as what?
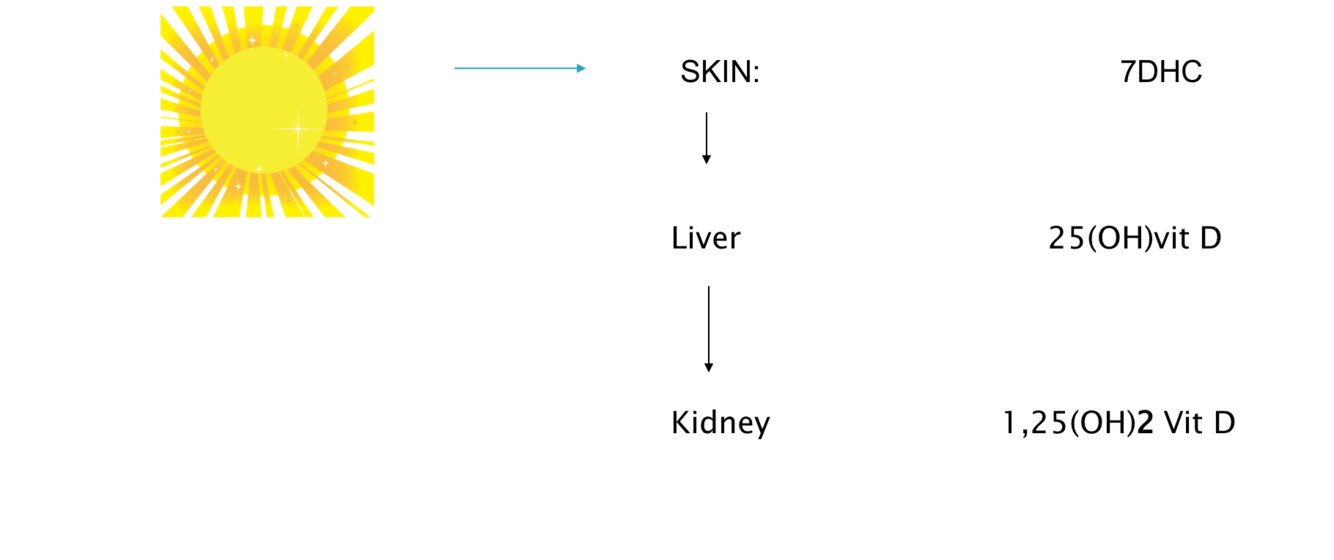
where does vitamin D come form and what is its function in the body?
Vitamin D comes from diet and sunshine
Vitamin D – absorption form the gut and there after works with parathyroid hormone to move calcium in and out of tissues and to store calcium
Low vitamin D happens in people with liver and kidney disease and people with darker skin due to competition with melanocytes
Harder for older people to make vitamin D
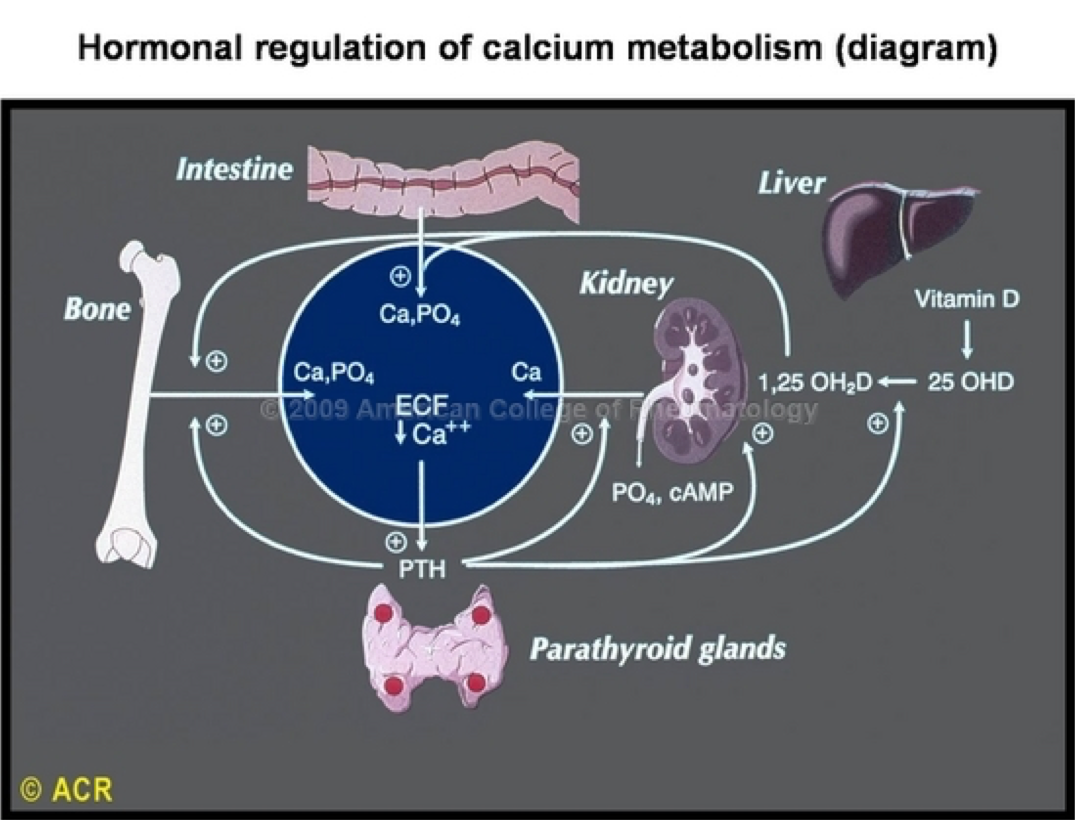
how is calcium regulated in the body and what is its function?
Maintaining extracellular fluid calcium within tight physiological limits as important for enzyme function, nerves to conduct or heart to beat
Calcium, moved in and out of cells, bone and kidney under action of parathyroid hormone
Kept under type limits
In liver or kidney disease this process may become impossible to maintain
Most stores are in bone
Paget’s Disease of Bone
what is pagets disease of bone?
Localised disorder of bone turnover
Increased bone resorption followed by increased bone formation
Leads to disorganised bone: bigger, less compact, more vascular and more susceptible to deformity and fracture
Paget’s disease of bone interferes with your body’s normal recycling process, in which new bone tissue gradually replaces old bone tissue. Over time, the disease can cause affected bones to become fragile and misshapen. Paget’s disease of bone most commonly occurs in the pelvis, skull, spine and legs
what is the cause of pagets disease?
Strong genetic component
15-30% are familial
Loci of SQSTMI
Restricted geographic distribution: those of Anglo-Saxon origins
Environmental trigger: Possibility of chronic viral infection within Osteoclast
what are the symptoms of pagets disease?
presents in a patient >40 years with bone pain occasionally presents with bone deformity, excessive heat over the Pagetic bone or by neurological complications such as nerve deafness
Always over 40 and normally over 60
Constant deep seated bone pain
Long bones, forearm bones, also pelvis and skull but can be any bone in the skeleton

what is the presentation of pagets disease?
Isolated elevation of serum alkaline phosphatase (on blood analysis) - is the commonest presentation in the 21st centuary
Bone pain and local heat
Bone deformity or fracture
Hearing loss
Rarely the development of osteosarcoma in affected bone
what is the Treatment of Paget’s Disease?
No evidence to treat asymptomatic Paget’s unless in skull or in area requiring surgical intervention
Do not treat based on a raised alkaline phosphatase alone
Intravenous Bisphosphonate therapy-One off zoledronic acid infusion
Conclusion:
Paget’s disease of bone is relatively common, particularly as a cause of isolated elevation of serum ________ phosphatase
Symptoms are most commonly bone ____ and sometimes bone deformity
___________ Paget’s disease can be safely ignored in most situations
It can be effectively managed when required using intravenous (or oral) ____________
alkaline
pain
Asymptomatic
Bisphosphonates
Rickets and Osteomalacia
what is Rickets and Osteomalacia?
Severe nutritional vitamin D or Calcium deficiency causes insufficient mineralisation and thus Rickets in a growing child and Osteomalacia in the adult when the epiphyseal lines are closed
Vitamin D stimulates the absorption of calcium and phosphate from the gut and calcium and phosphate then become available for bone mineralisation
Muscle function is also impaired in low vitamin D states
Same disease, depends on age of sufferer
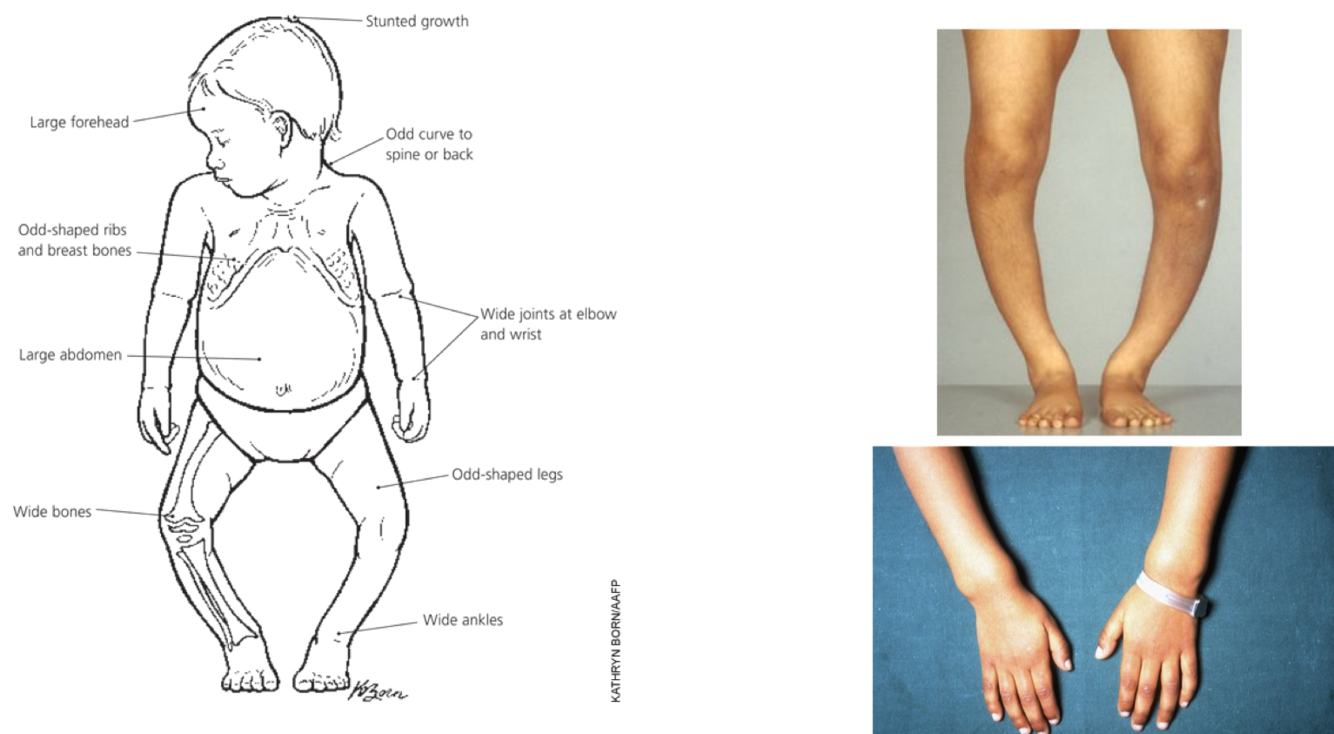
how does Rickets present in a child?
stunted growth
Abnormal bone growth
Boing of leg bones
Large abdomen
Odd shaped ribs
Rare in UK due to nutritional problems
Simply treated with calcium and vitamin D supplements
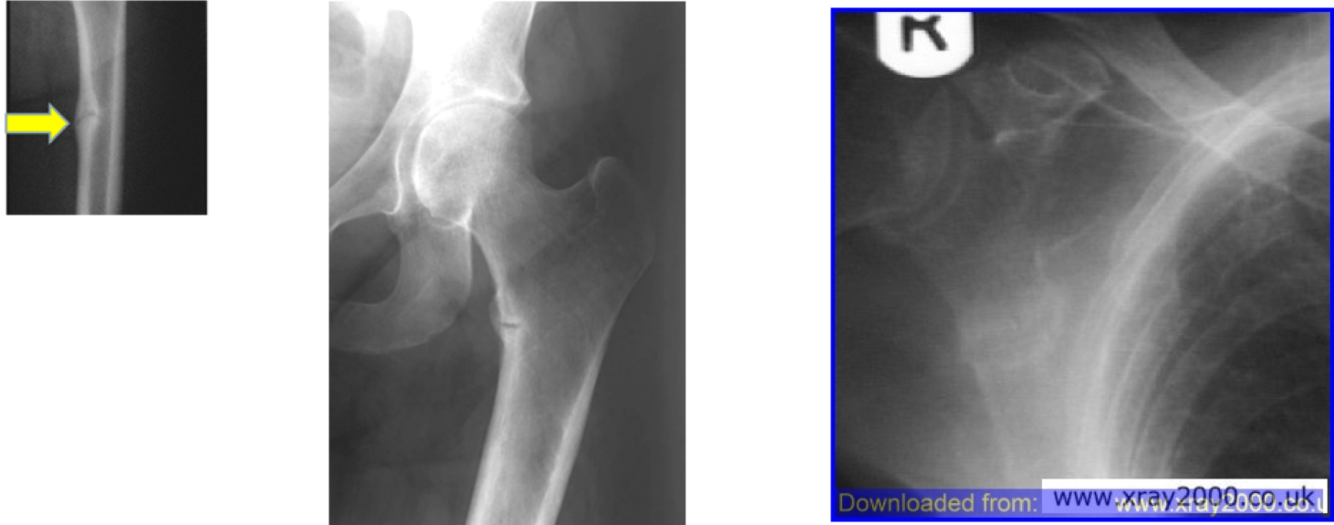
Osteomalacia - who is it common in, what is the symptoms and what is the treatment?
Common in elderly
Symptoms: bone pain, muscle weakness, increased falls risk
May see micro fractures on x-ray – lucre zones
Calcium and vitamin D supplements for treatment
Osteogenesis Imperfecta
what is Osteogenesis Imperfecta?
Genetic disorder of connective tissue characterised by fragile bones from mild trauma and even acts of daily life
Other non bone clinical features - Genetic abnormality of type 1 collagen and Type 1 collagen in other tissues
Broad clinical range from those which are prenatally fatal to those only presenting in 40s with early ‘osteoporosis’
what are the types of OI?
Defects in type 1 collagen-eight different types exist-first 4 most common
Type 1: milder form-when child starts to walk and can present in adults
Type 11: lethal by age 1 (most severe)
Type 111: progressive deforming with severe bone dysplasia and poor growth
Type 4 : similar to type 1 but more severe
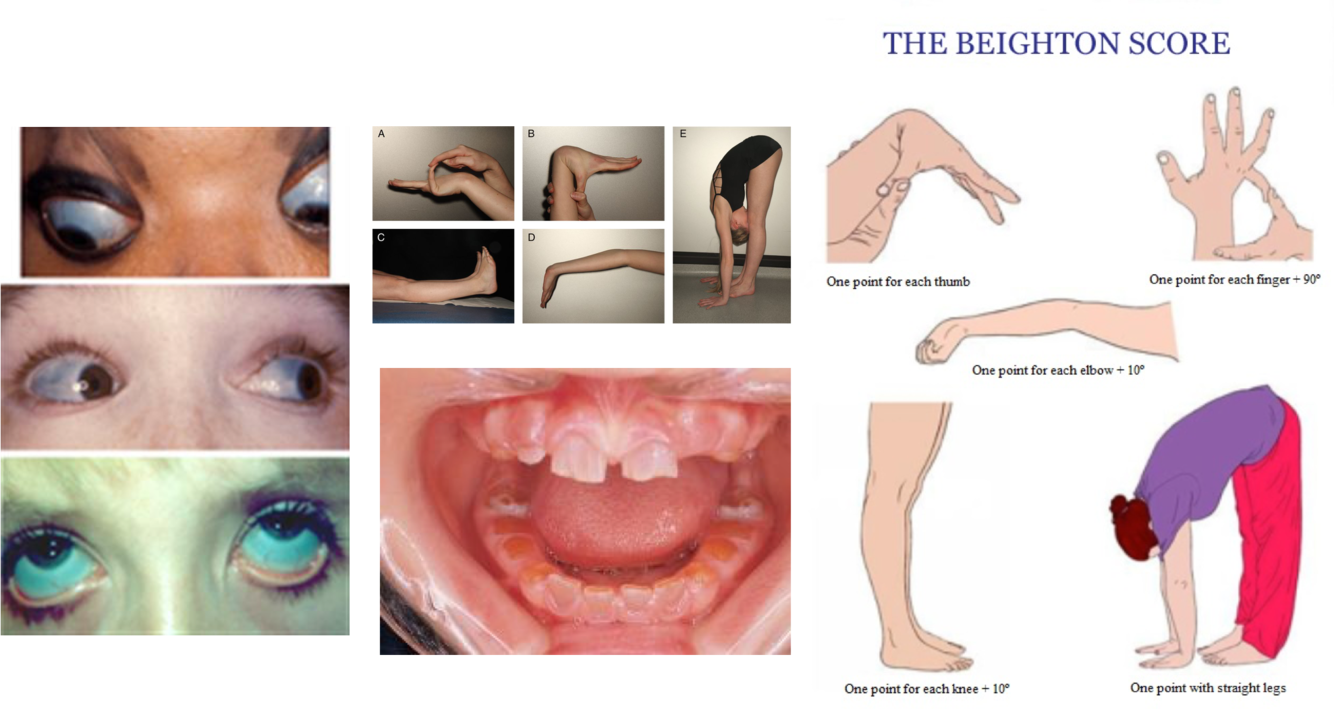
Osteogenesis Imperfecta - what are some other features?
Growth deficiency
Defective tooth formation (dentigenesis imperfecta)
Hearing loss
Blue sclera
Scoliosis / Barrel Chest
Ligamentous laxity
Easy bruising
what is the Management of OI?
Surgical - to treat fractures
Medical - to prevent fracture, intravenous Bisphosphonates
Social - educational and social adaptions
Genetic - genetic counselling for parents and next generation
Osteoporosis
Rest of lecture on this
Commonest metabolic bone disease
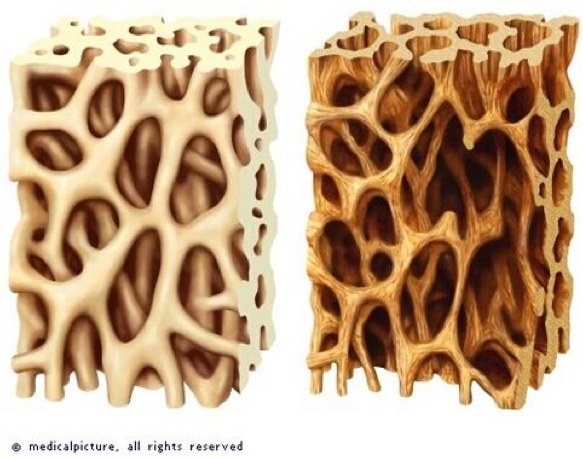
what is osteoprosis?
A metabolic bone disease characterised by low bone mass and micro architectural deterioration of bone tissue, leading to enhanced bone fragility and a consequent increase in fracture risk
A result on DXA bone scanning <-2.5 SDs below the young adult mean in a post menopausal woman ( T-score)
osteoprosis is all about what?
Relevance of osteoporosis is risk of fracture
Risk of fracture related to: Age; BMD; Falls; and Bone Turnover
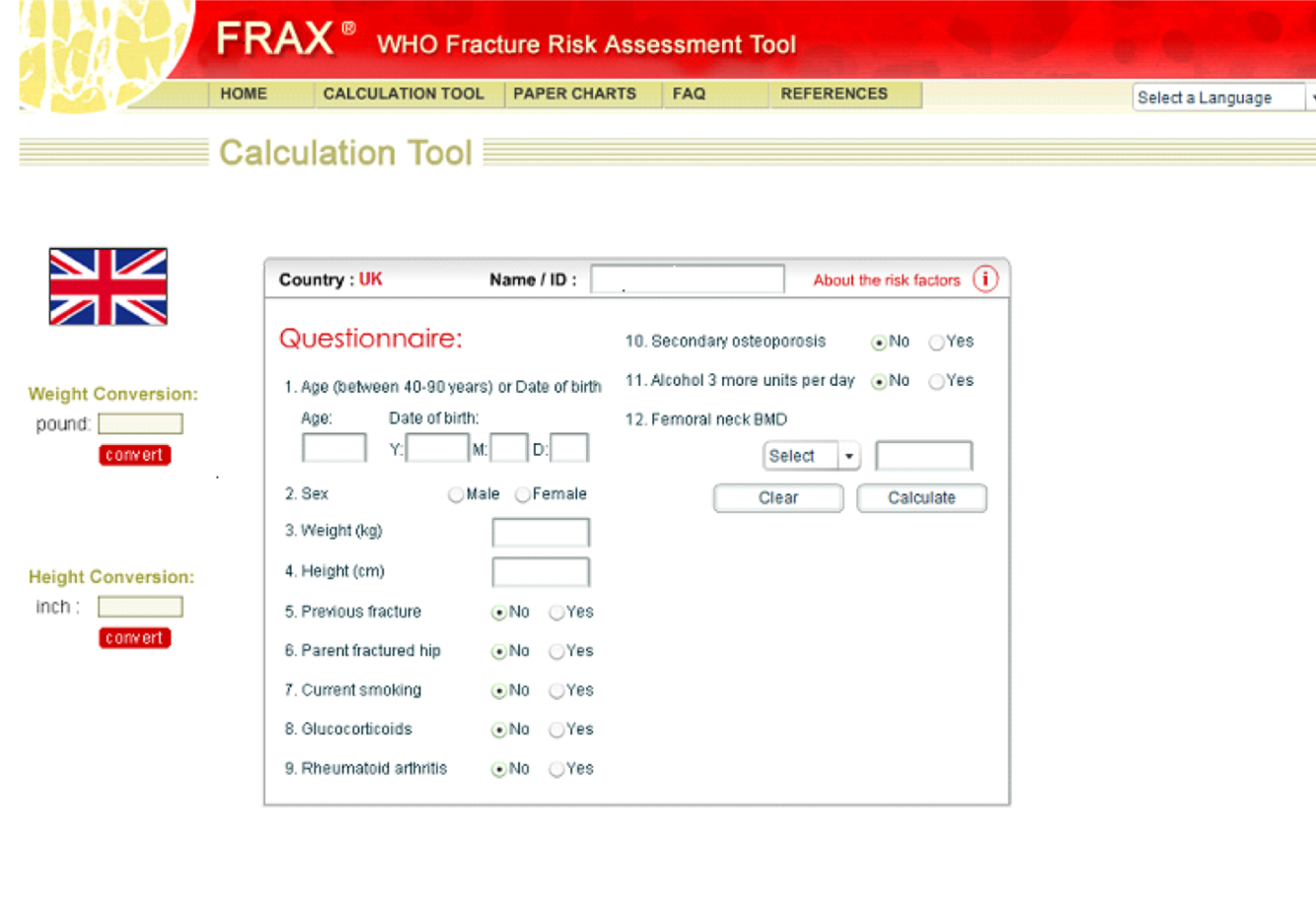
Picture showing - Fracture assessment risk tools












-
Joints and Synovial Fluid and Cartilage33
-
Pre-Practical Lecture – Upper Limb41
-
Embryology23
-
Bone and Soft Tissue Infection60
-
Bone and Soft Tissue Tumours59
-
Anatomy of the Shoulder and Elbow24
-
Anatomy of the Hand and Wrist6
-
Orthopaedic problems of the Hand31
-
Musculoskeletal Growth/Injury and Repair - Nerve31
-
Musculoskeletal Growth/Injury and Repair - ligament injuries6
-
Musculoskeletal Growth/Injury and Repair - tendon injuries18
-
Musculoskeletal Growth/Injury and Repair - bone growth and fracture healing25
-
Nerve Palsies in the Limbs44
-
Introduction the Rheumatology and Rheumatoid Arthritis28
-
The Science of Rheumatoid Arthritis25
-
Clinical Aspects of RA and Approach to Therapeutics12
-
Rheumatoid Arthritis: A patient’s journey7
-
Metabolic Bone Disease48
-
Commonly encountered rheumatic diseases: crystal arthropathies & polymyalgia rheumatica39
-
Seronegative Arthritis35
-
Mini Symposium: Multi-system Autoimmune Disease52
-
Shoulder and Elbow Problems26
-
Osteoarthritis and Principles of Management22
-
Juvenile Idiopathic Arthritis45
-
Anatomy of the Hip and Knee - Clinical47
-
Anatomy of the Hip and Knee47
-
Anatomy of Lower Leg, Ankle and Foot26
-
Orthopaedic Hip Conditions51
-
Principles of Paediatric Orthopaedics20
-
Children’s Orthopaedics – ‘The Big 3’ - DDH, Perthes’ Disease, SUFE33
-
Children’s Orthopaedics – The Limping Child40
-
Children’s Orthopaedics - Complex needs - CP, Talipes,Scoliosis48
-
Foot Problems83
-
Orthopaedic Knee Conditions39
-
Mini Symposium: Spine (Degeneration, Low Back Pain, Disc Prolapse)40
-
Mini Symposium: Introduction, Spinal Injuries and Cases50
-
Forensic Aspects of Trauma 124
-
Forensic Aspects of Trauma 218
-
How to Describe a Fracture31
-
Basics of Fracture Management38
-
Paediatric Trauma (including NAI)38
-
Upper Limb Injuries34
-
Mini Symposium: The Multiply Injured Patient28
-
Mini Symposium: Fractures 1 (Basics, healing and complications) - Open fractures21
-
Mini Symposium - Fractures 1 (Basics, healing and complications) - Dislocations15
