Mini Symposium: Spine (Degeneration, Low Back Pain, Disc Prolapse) Flashcards
(40 cards)
what is the most common form of disc prolapses?
Normal spinal cord finishes at a level of above L1 and below that we just have spinal roots
Most common form of disc prolapses is lateral but occasionally central can be seen which causes different symptoms

what type of joint are Intervertebral Discs?
Secondary Cartilaginous Joint
what is the structure of the intervertebral discs?
- Disc is largest avascular structure in the body
- Annulus fibrosus - Tough outer layer
- Nucleus pulposus - Gelatinous core
- Annulus may tear and nucleus prolapse - Can cause cord/nerve root compression

- Cartilaginous end plate of each disc attaches to bony endplate of ________
- The ___ and ___ connect discs with vertebral bodies
- The fibres of the annulus fibrosis (collagen) run ________ and alternately between layers
- They resist ________ movements
- Discs fail with _______ movements
vertebra
ALL and PLL
obliquely
rotational
twisting

what make sup the inververtebral disc?
- The nucleus pulposus consists mainly of water - 88%
- collagen & proteoglycans (very hydrophilic)
- The disc is kidney bean shaped
Disc prolapses are usually __________
postero-lateral

what happens to the intervertebral discs as part of the normal ageing process?
- Decreased water content of discs (see this on MRI)
- Disc space narrowing
- “Degenerative” changes on X-rays
- Degenerative changes in the facet joints
- Aggravated by smoking, etc.
what are some different Pathological Processes?
- Tearing of annulus fibrosis and protrusion of the nucleus
- Nerve root compression by osteophytes
- Central spinal stenosis
- Abnormal movement (between vertebra)
- Spondylolysis
- Spondylolisthesis
what is nerve root pain like?
- Fairly common
- Limb pain worse than back pain
- Pain in a nerve root distribution (radicular)
- Root tension signs (sciatic nerve stretch test)
- Root compression signs
- Dermatomes & myotomes
what does radicular mean?
Pain in a nerve root distribution
what is the management of nerve root pain?
- Most will settle, about 90% in 3 months (without surgical intervention)
- Physiotherapy
- Strong analgesia
- Referral after 12 weeks
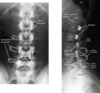
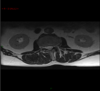
- Imaging - MRI (this is the modality of choice)
MRI Scans showing disc prolapse in the second one and first is normal
Spinal canal boundaries:
Anterior – vertebral body
Posterior – laminar and facet joints posteriorly


whata re the different kinds of disc problems?
- Bulge (generalised) – common, majority asymptomatic, relevance?, nucleus contained, annulus slightly buldging
- Protrusion (annulus weakened but still intact)
- Extrusion (through annulus but in continuity)
- Sequestration (dessicated disc material free in canal)

what regions do disc prolapses most often occur?
Lumbar > cervical > thoracic
wher eis a Cervical Disc Prolapse most common?
Most commonly C5/6

how often and where do thoracic disc prolapses occur?
- <1% of intervertebral disc prolapses
- Mid to lower levels (75% T8-12)
- Most at T11/12
- Central, posterolateral and lateral herniations
where do lumbar disc prolapses occur?
- Usually L4/5 (45%), followed by L5/S1 (40%), then L3/4 (10%)
- Most are posterolateral - (Posterior Longitudinal Lig weakest)
L3/4 – femoral neuralgia, pain on the anterior of the thigh
L5/S1 – symptoms are pain going right down the leg into the foot and
what may central fisc prolapses in the lumbar region cause?
Central disc may give pain in both legs, or may be back pain only
Prolapsed Lumbar Inter-Vertebral Disc - summary table
EHL - extensor hallucis longus

what is Cauda Equina Syndrome?
Compression of cauda equina
sacral nerve roots compressed – can result in permanent bladder and anal sphincter dysfunction and incontinence

what is the treatment of cauda equina syndrome?
Cant be treated conservatively
Need to treat rapidly
• Surgical emergency - admission, urgent MRI scan, emergency operation within 48h of onset; delay results in permanent dysfunction
what is the aetiology of cauda equina syndrome?
central lumbar disc prolapse (commonest)
tumours
trauma (burst or Chance #, disc) or spinal stenosis
infection (epidural abscess – rare in this country)
iatrogenic (spinal surgery or manipulation, spinal epidural injection)
whata re the clinica features of cauda equina syndrome?
Injury or precipitating event
Location of symptoms (bilat buttock & leg pain + varying dysaethesiae + weakness – beware)
Bowel or bladder dysfunction (urinary retention +/- incontinence overflow)
PR exam - saddle anaesthesia (perianal loss of sensation), loss of anal tone & anal reflex
High index of suspicion in spinal post-op patients with increasing leg pain in presence of urinary retention

in cauds erquina syndrome is there a Delay in diagnosis?
•Shapiro (USA) – average delay 9 days
–4 patient related
–20 physician related!!
•Surgical emergency