How is O2 transported in the body?
O2 binds to Hbg sites (has preferential binding).
Dissolves in blood
What effect will giving more O2 to a person will 99% sats have?
No effect. Site are already at max capacity.
What is the normal PaO2?
80mmHg
What happens to PaO2 as HbO2 drops?
Decreases. O2 will preferentially bind to HgB. If it isn’t binding to HgB then it won’t stay in blood
What factors affect HbO2 binding? How do they affect?
- pH - <7.4 saturation binding decreases
- temp - Increasing temp decreases binding abilities
- Diphosphoglycerate (DPG) increases presence decreases O2 binding
What is a Bohr shift?
Shift to the right of the O2 dissociation curve
How does DPG decrease O2 binding? What causes increased levels of DPG
DPG binds to Hbg instead of O2.
Increase temp, thyroid hormone, testosterone and epinephrine raise DPG
What is Meconium? How does it influence fetal ARDs?
Meconium is fetal feces; if it enters the amniotic fluid it can contaminate it. In late gestation, the baby starts fetal breathing movements (FBM)s which can draw amniotic fluid into the lungs. Contaminated fluid can cause inflammation leading to hyaline inflammatory disease
What is ARDS?
Acute Respiritory Distress syndrome
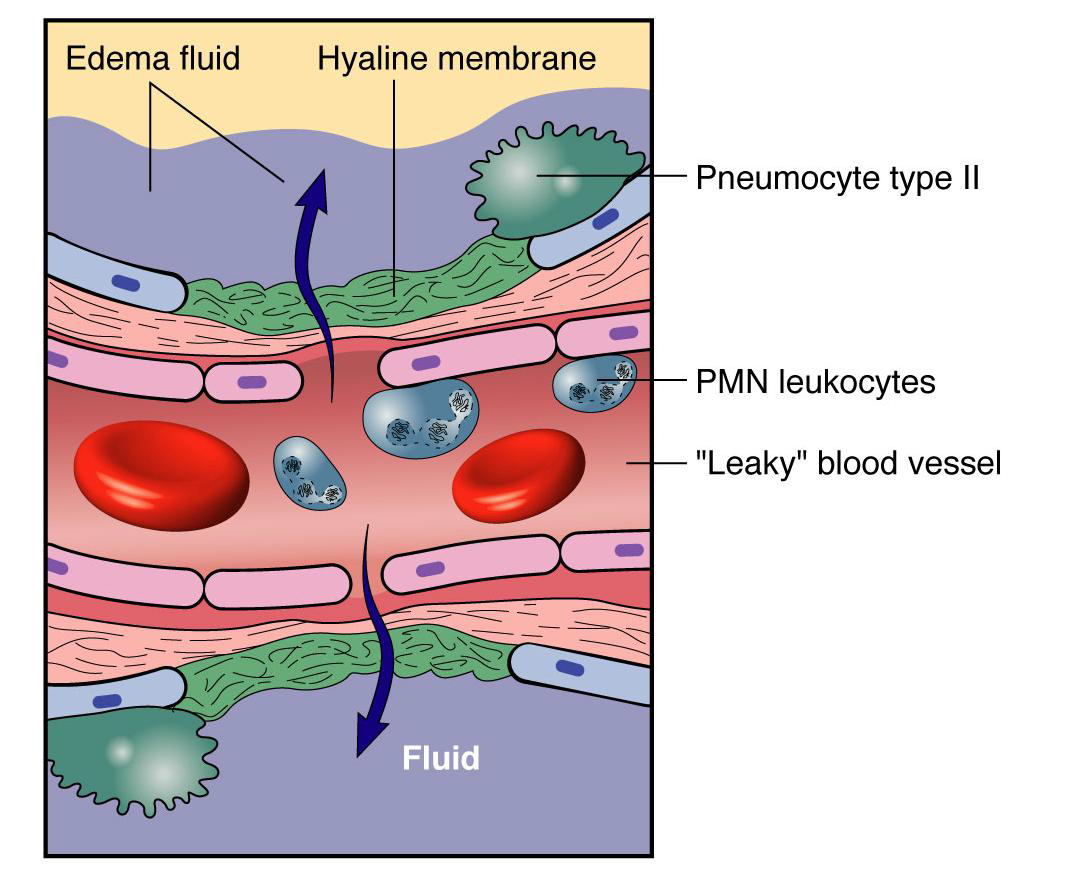
What is the pathophysiology of ARDS?
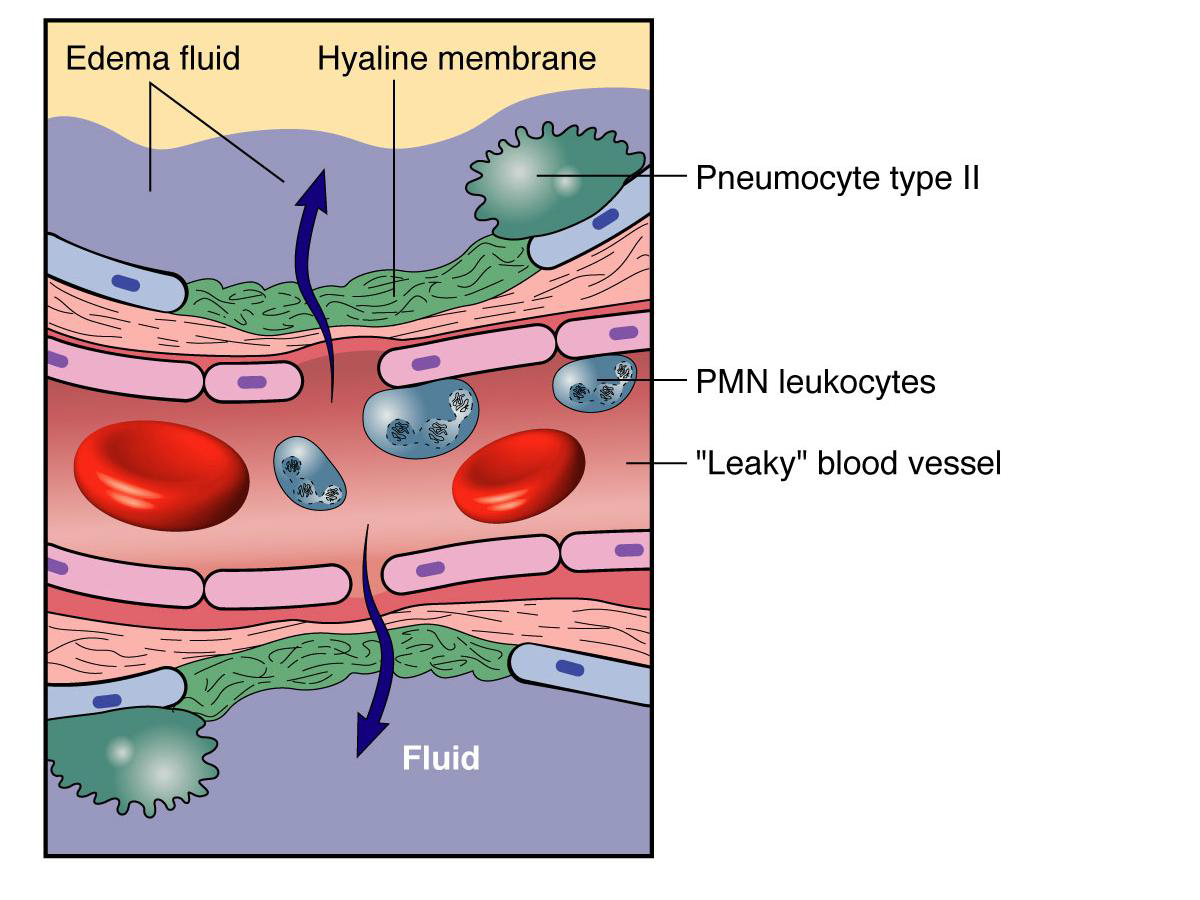
Foreign particles / substances enter the alveoli (soot, pollutants) causing injury to type I epithelial cells. Neutrophiles enter and release inflammatory mediators and proteolytic enzymes. Causes hyaline membrane disease (thickening of injured area). Thickened area + fluid in alveoli = decreased diffusion in the area
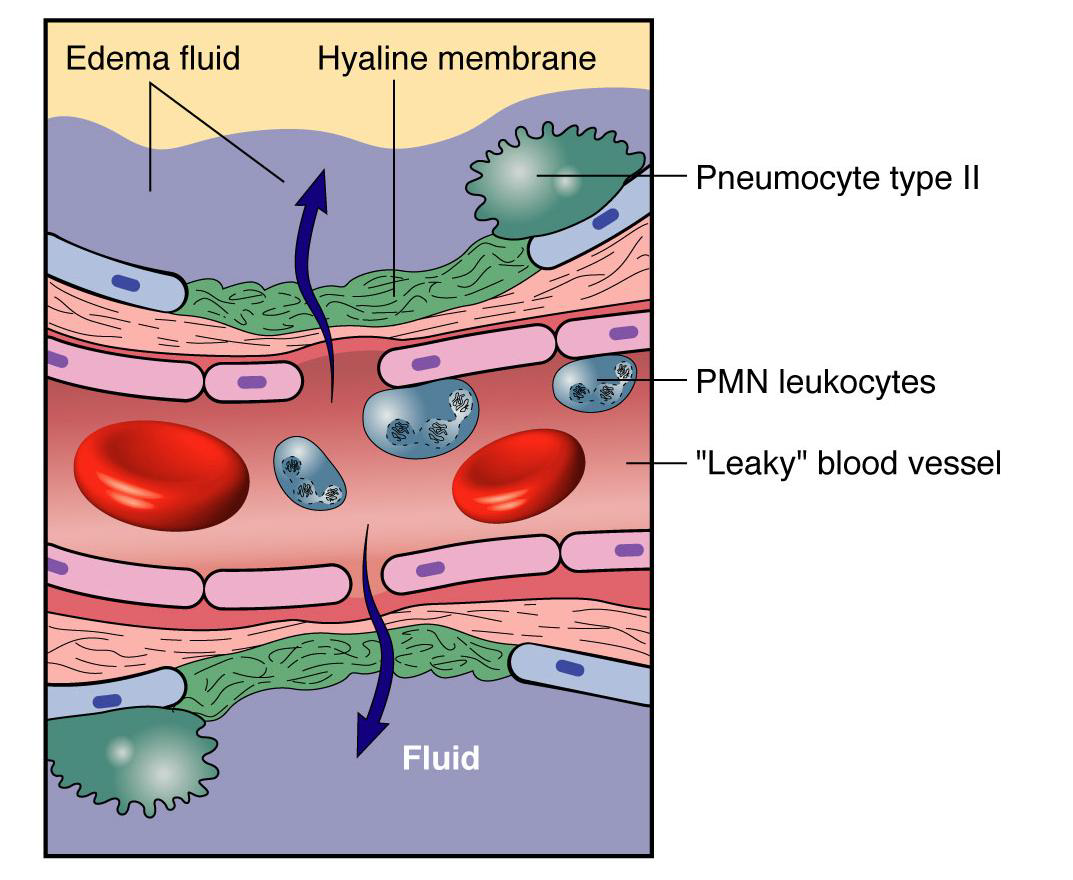
What is hyaline membrane disease?
Inflammation of the basment membrane where damage to the epithelium was. Causes exposed basement membrane to thicken = decreased diffusion
What are manifestations of ARDS? Clinical consequences?
Manifestations:
- Leaky capillaries which lead to non cardiogenic edema
- Destruction of Type II alveoli cells causing atelectaisis
- Inflammation dt injury which causes fibrosis
Results in increased WOB, shunting (with alveoli collapsed, blood gets shunted elsewhere), hypoxemia
What is noncardiogenic pulmonary edema?
Pulmonary edema dt non CHF reasons (exudate following WBCs into lung)
What is patho cystic fibrosis?
Recessive disorder in individuals lacking the Cystic fibrosis transport regulator (CFTR) which causes a decrease in transport of Cl- watery solution. Without this solution the mucous sticks to the cillia in the bronchials..
The mucous forms a culture medium for bacteria growth causing recurrent infections
What are ways to management of CF?
Gene therapy, lung transplant, patthing person on the back, suctioning
What body parts does CF affect? What are possible S&S?
Respiritory: decreased air conductance
Pancreatic and bilary ducts: digestive problems, flatulence, steatorrhea, weight loss
What micro-organisms can cause respiritory tract infections?
Bacteria, viruses, mycosis, mycoplasma
What is typical pneumonia?
aka alveolae pneumonias. Dt bacteria
Infection attracts PMNs into alveolar lumen which produces exudate. Exudate causes respiritory distress
Cap endothelium breaks causing RBCs to enter alveoli - blood in sputum
Likely to have productive cough
What is atypical pneumonia?
aka interstitial pneumonia dt viruses
Alveoli lumen is clear. WBC enter alveoli walls though blood vessels. Edema builds up in walls
Increased thickness of walls decreases diffusion
Produces non productive cough
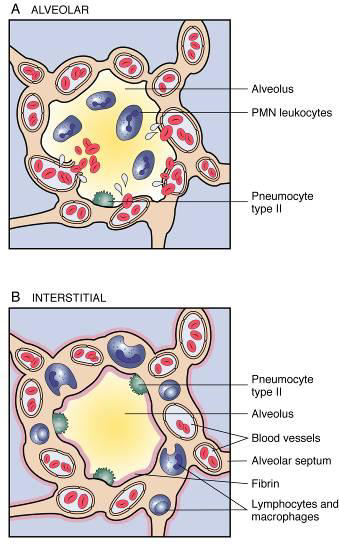
Differences between alveolar and interstitial pneumonias?
Alveolar
- fluid is in the alveoli
- RBC + WBCs in alveoli
- Productive bloody cough
- caused by bacteria
Interstitial:
- fluid is in interstitial walls
- alveoli lumen are clear
- non productive cough
- caused by viruses
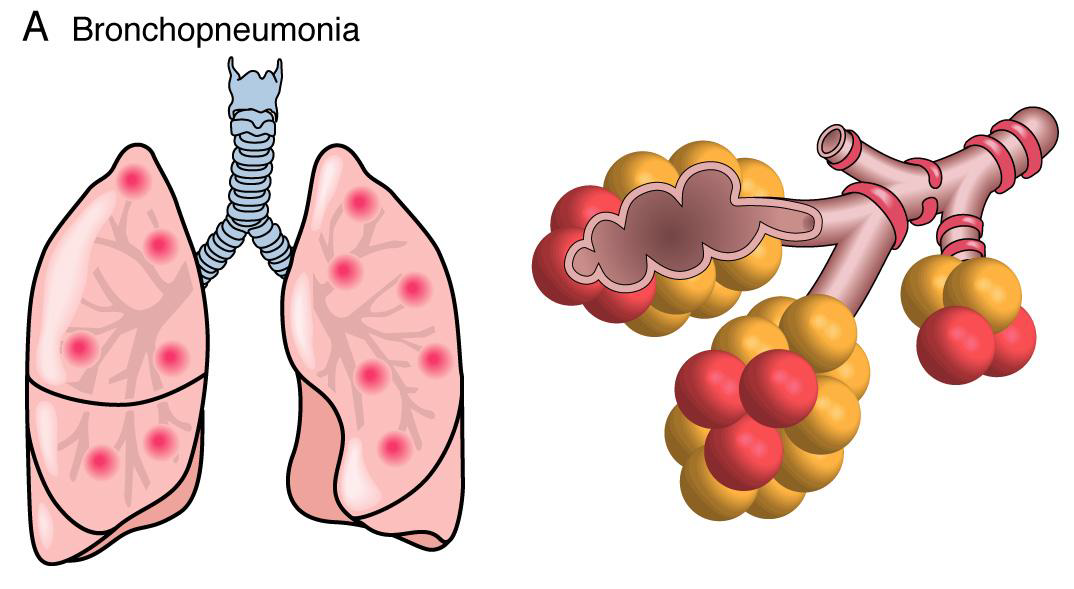
What is bronchopneumonia? S&S?
Patchy distribution throughout both lungs. Diffuse.
S&S: Chills, fever, increased peripheral resistances, increased resp rate, bronchial breathing (gas exchange in the bronchi), purulent and bloody sputum. Severe chest pain and abdominal distension)
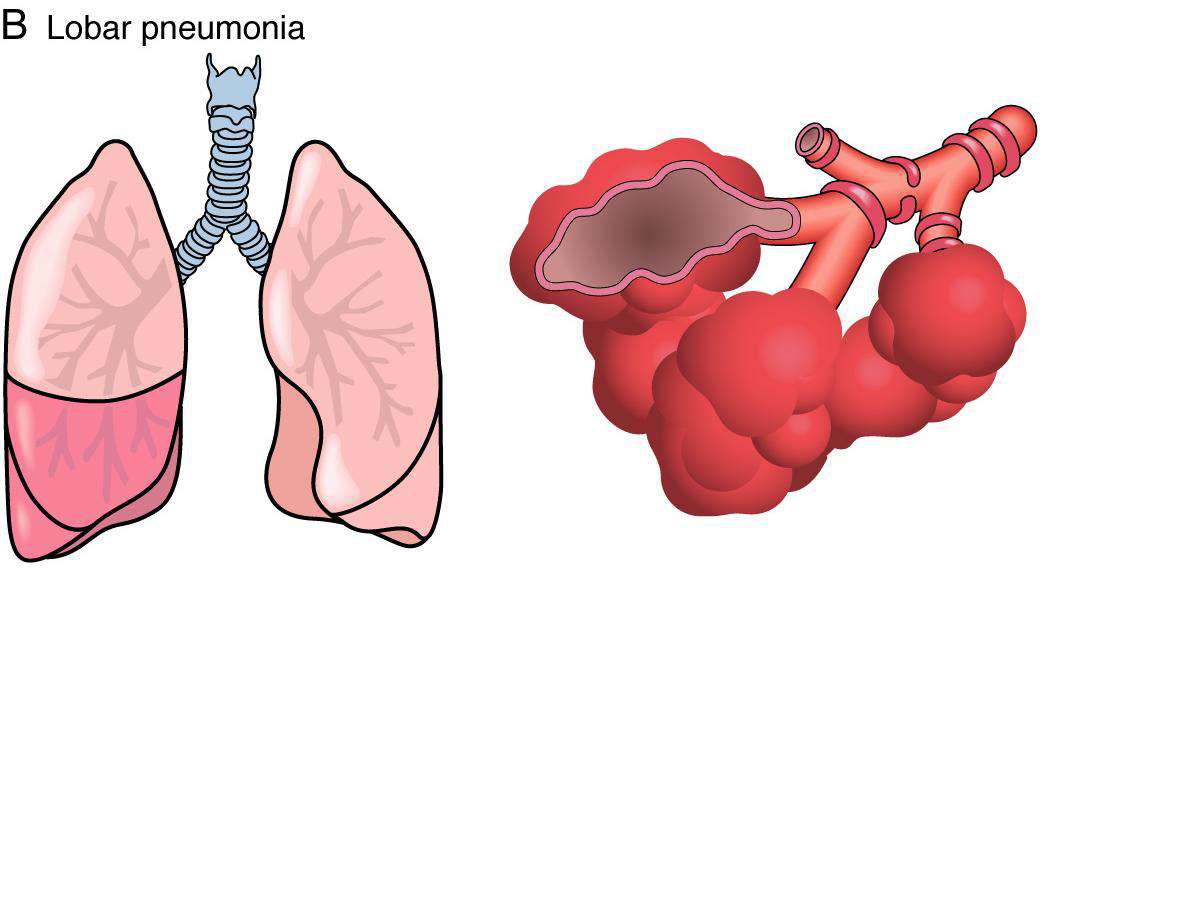
What is lobar pneumonia? what are clinical manifestations?
Pneumonia in one lobe of lung. All the alveoli are infected. Associated with consolidation of lobe.
S&S: Shallow breathing, cyanosis, pleurisy (pleuritis), N&V, rust colored sputum, fever, chills
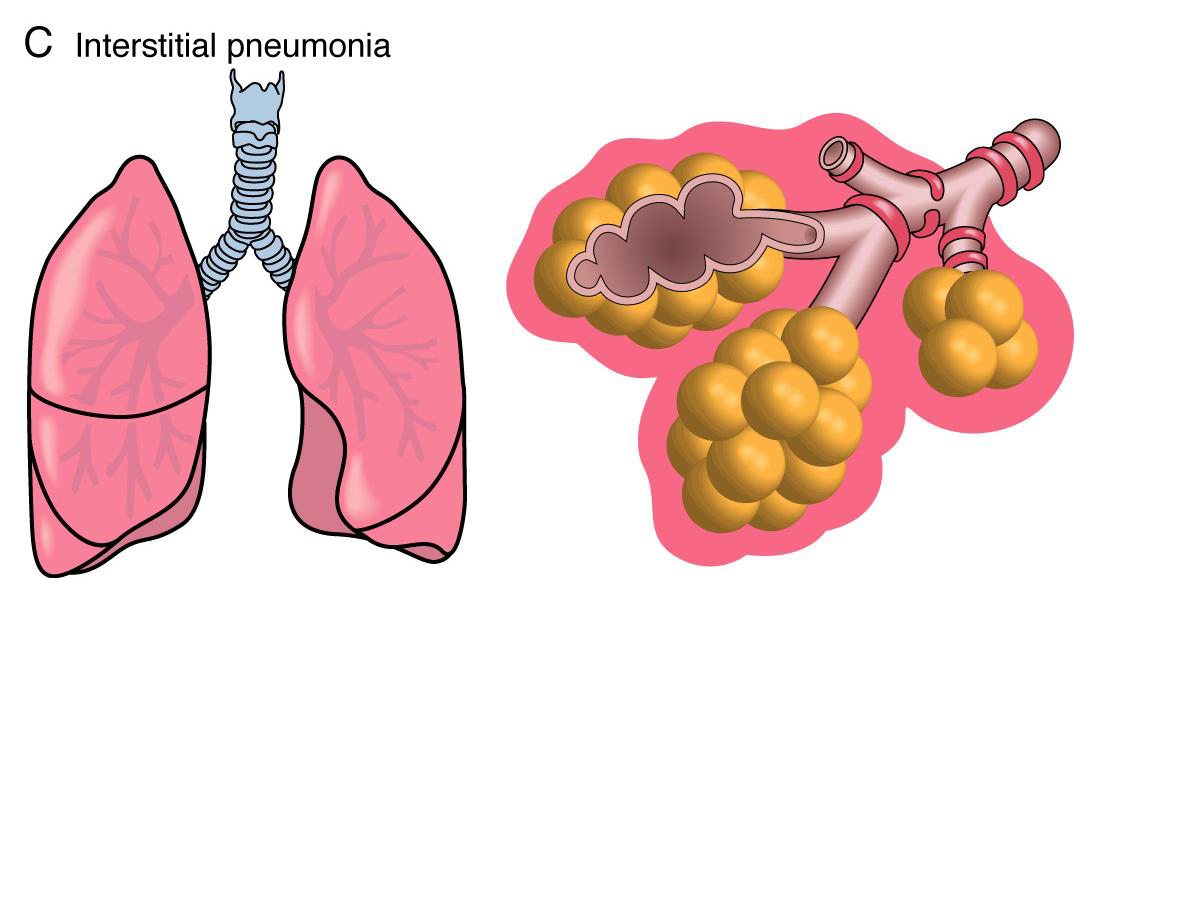
What is interstitial pnemonia? Clinical manifestiation?
Widespread disttribution. Diffuse inflammation dt viral infeciton. Walls are inflitrated with WBCs which increase septum width
S&S: cyanosis, fever, chills, alveolar wall fibrosis, non productive cough, finger clubbing (severe)
Why is the right lower lobe most often implicated with lobar pneumonia?
Rt bronchus is more vertical dt the position of the heart than the lt bronchus. Makes Pathogens more likely to enter and settle










