When do Bartholin cysts typically present?
During reproductive years
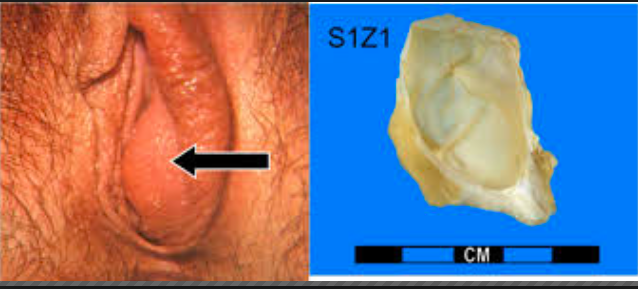
What is a condyloma?
any warty neoplasm of vulvar skin
What are the two types of condyloma?
Condyloma acuminatum (HPV 6/11)- below
Condyloma lata (secondary syphillis)

What is this?
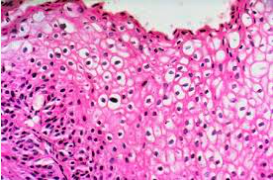
Koilocytes, commonly seen in HPV induced condylomas
T or F. Condylomas rarely progress to carcinoma
T. (6 and 11 are low risk)
What is Lichen sclerosis?
A marked thinning of the vulvar epidermis, combined with fibrosis (sclerosis) of the dermis that presents are a white parchment-like patch (aka leukoplakia)

When is lichen sclerosis most commonly seen?
post-menopausal women
What causes lichen sclerosis?
autoimmune
What is the prognosis for lichen sclerosis?
Benign, BUT associated with a slightly increased risk for squamous cell carcinoma transformation
What is lichen simplex chronicus?
Hyperplasia of the vulvar epithelium that presents as leukoplakia with thick, leathery vulvar skin that is pruritic

What is the prognosis of lichen complex chronicus?
Benign, with no increased risk of squamous cell carcinoma transformation
Describe vulvar carcinomas
These are carcinomas arising from the vulvar squamous epithelium that are relatively rare and require biopsy
What are the associated causes of vulvar carcinoma?
Can be HPV or non-HPV related. Risk factors include HPV, multiple sex partners, and early first age of intercourse
When does vulvar carcinoma most commonly occur?
reproductive age
What is the cellular precursor of vulvar carcinoma?
Vulvar intraepithelial neoplasia (VIN) marked by increased mitotic activity, nuclear atypia, and koilocytic change
Non-HPV related vulvar carcinoma most commonly arises from what?
long-standing lichen sclerosis (generally seen in 70+ yo women)
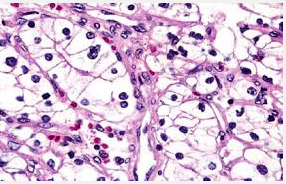
What is extramammary Paget disease?
Malignant epithelial transformation of the vulva that present as very erythematous, pruritic, ulcerated skin

T or F. Extramammary Pagets is not associated with an underlying carcinoma
T. While Mammary Paget’s disease is typically

Its important to distinguish extramammary Paget’s from what?
Vulvar melanoma
How can extramammary paget’s be dsitinguished from vulvar melanomas?
Paget cells are PAS+, keratin +, and S100- while
Melanoma is PAS+, keratin -, and S100+
What is vaginal adenosis?
This is a focal persistance of columnar epithelium in the upper vagina where typically squmous epithelium from the lower vagina grows upward to replace
This is benign but can be precancerous to a clear-cell adenocarcinoma

Vaginal adenosis is more common in what pop?
Those exposed to Diethylstillbestrol in utero
What causes clear cell adenocarcinoma?
This is a rare complication of DES-induced vaginal adenosis
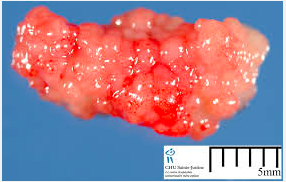
What is an embryonal rhabdomyosarcoma?
Malignant proliferation of mesenchymal tissue of immature skeletal tissue that presents as a grape-like red external swelling of vaginal area in infants (aka sarcoma botyoides)






-
Female Anatomy Review48
-
Genetics of Sex Determination24
-
Male Anatomy Review10
-
Costanzo Ch. 1060
-
Female Hormones46
-
Male Hormones31
-
Female Puberty51
-
The Menstrual Cycle46
-
Costanzo Ch. 10 (2)20
-
Breast Pathology Pre-Study98
-
Cervix Pathology Pre-Study71
-
Male Puberty31
-
Disorders of Sexual Differentiation56
-
Tx of Breast and Endometrial Cancer58
-
Tx of Ovarian and Bladder Cancer22
-
Ovarian Pathology49
-
Tx of BPH30
-
Tx of Testicular Cancer23
-
Tx of Prostate Cancer32
-
Sperm Storage, Transport, and Male Sexual Dysfunction23
-
Endometrium Pathology54
-
Male Pathology81
-
Syphilis17
-
Trichomonas5
-
Mullerian Duct Abnormalities17
-
Inhibin and Actvin9
-
Diagnosing Disorders of sex hormones4
-
Pathoma Female67
