Session 2 Flashcards
(32 cards)
Identify definitions of disability and their implications
- You’re considered disabled under the Equality Act 2010 if you have a physical or mental impairment that has a ‘substantial’ and ‘long-term’ negative effect on your ability to do normal daily activities e.g. it takes much longer than it usually would to complete a daily task like getting dressed and ‘long-term’ means 12 months or more.
- WHO definition: disabilities is an umbrella term, covering impairments, activity limitations, and participation restrictions. An impairment is a problem in body function or structure; an activity limitation is a difficulty encountered by an individual in executing a task or action; while a participation restriction is a problem caused by an individual in involvement in life situations
- Implications: disabled people may find it more difficult to get or keep hold onto a trouble, difficult getting about on public transport, difficult socializing and doing hobbies. They may face discrimination.
Identify barriers for people with disabilities in accessing healthcare
Physical/environmental barriers (e.g. accessibility of the GP surgery)
- Suitable parking bays
- Wheelchair ramp availability
- Whether Guide dogs or other assistance dogs are allowed
- Life availability
- Height of the registration counter (for wheelchair bound people)
- Narrow corridors
- Announcement systems which are both visual and audio for deaf and/or blind people
Attitudinal and behavioural barriers (e.g. the way staff treat disabled patients)
- Some staff talk down to people – assume that a physical disability also comes with a mental disability
- Some staff might not be aware of the disability – e.g. deaf or visual impaired or of autism
- Some staff might speak more to the carer or parent or other person present rather than to the patient
- Some staff might come across as patronizing / impatient / brisk – not wanting to take the time to figure out the patient’s competence, assuming incompetence
Institutional barriers (e.g. policies and staff training at the GP surgery)
- Give staff training to be aware of hidden disabilities, how to judge competence and ability to give consent
- Aids such as wheelchairs or Braille documents or sign language interpreters may not be available on site
- Give staff training about how to deal with disabled people in a supportive yet non-patronizing way.
Define health related behaviour
- Anything that may promote good health or lead to illness e.g. smoking, drinking, drug use, taking exercise, eating a healthy diet, safer sex behaviour, taking up screening activities, adhering to treatment regimes etc.
- There is huge concern about behaviour because at least 1/3 of all disease burden is caused by tobacco, alcohol, blood pressure, cholesterol and obesity
- Behaviourial risk factors including tobacco use, physical inactivity and unhealthy diet, are responsible for about 80% of coronary heart disease and cerebrovascular disease. Smoking is estimated to cause about 71% of all lung cancer deaths, 42% of chronic respiratory disease and nearly 10% of cardiovascular disease
What are the theories to help understand people’s health-related behaviour?
- Learning theories: classical conditioning, operant conditioning and social learning theory
- Social cognition models: health belief model and theory of planned behaviour
- Stages of change model
Explain about classical conditioning
- Classical conditioning e.g. food -> salivation, food + bell -> salivation, bell -> salivation (Pavlov dog). Behaviours can become linked to unrelated stimuli (LEARNING BY ASSOCIATION). In humans, many physical responses can become classically conditioned e.g. anticipatory nausea in chemotherapy, phobias e.g. fear of hospital (unconscious association)
- Behaviours such as smoking, drinking can become unconsciously paired with environment (e.g. work break) or emotions (e.g. anxiety).
- Conditioned behaviours can become habit
- Negative associations: Aversive techniques in smoking / alcohol misuse = pair behaviour with unpleasant response. E.g. alcohol + medication to induce nausea (nausea is result of medication + alcohol but comes to be associated with alcohol (CR)) therefore people are less like to engage in this particular behaviour
- Smoke holding e.g. finding something else to do such as going for a jog or yoga.
- Break unconscious response – elastic band on cigarette packet! This adds an extra step so now the decision is a now conscious one.
How may classical conditioning play an important role in placebo effects?
Our understanding of classical conditioning can be used to reduce symptoms or induce positive physical responses.
E.g. we know that physical symptoms are more easily conditioned in response to novel food or liquid.
We also know that once conditioning has occurred it can block a third stimulus becoming conditioned. Research has confirmed that giving chemotherapy patients a novel drink before each chemotherapy infusion prevents anticipatory nausea and even shortens the time that nausea is experienced during chemotherapy because they associate nausea with the drink and not the hospital context.
This has also been demonstrated with allergy symptoms. If people are given a novel drink just before taking antihistamine drugs for five days, the drink alone will start to trigger the same drop in basophil activity and improvement in symptoms as the antihistamine drug.
Classical conditioning therefore plays an important role in placebo effects and may underpin many of the effects of alternative therapies.
Explain about operant learning
- Operant learning: people/animals act on the environment and behaviour is shaped by the consequences (reward or punishment). Behaviour is reinforced (increases) if it is rewarded (positive outcome) or a punishment is removed. Behaviour decreases if it is punished (negative outcome) or a reward is taken away. ASSOCIATIONS BETWEEN ACTIONS AND THEIR CONSEQUENCES.
- It is a key way we learn all the time – behaviour shaped by rewards and punishments.
- However the reward or punishment needs to occur within a short time period of the behaviour for this unconscious association to be made.
- Primary reinforcers are those needed for survival, suc as water, food, sleep and sex.
- Secondary reinforcers are those that acquire value through experience, such as money, praise and attention.
- Variable ratio patterns of reinforcement lead to the strongest responses and are hardest to extinguish. This may explain why gamblers find it so hard to stop. It also has repercussions for drug abuse treatment. For example methadone blocks the positive effects of heroin but if it is used intermittently and the drug gets occasional highs from heroin they are on a variable ratio pattern on reinforcement and may find it even harder to stop.
- Problem is unhealthy behaviours are immediately rewarding (alcohol, smoking, chocolate, unsafe sex) so behaviour can be driven by short-term rewards. The short term rewards at the time seem to far out-weigh any long term consequences.
- Operant conditioning and changing health behaviour: shape behaviour through reinforcement (punishment or reward) e.g. money saved towards holiday by giving up smoking.
What are the limitations of conditioning theories?
- Classical and operant conditioning based on simple stimulus-response associations.
- No account of cognitive processes, knowledge, beliefs, memory, attitudes, expectations etc (how we think, how we make decisions consciously)
- No account of social context (how we are influenced by people around us)
Describe the Social Learning Theory
- people can learn vicariously (observation/modeling) – by learning from the consequences of other people’s behaviour and applying it towards themselves.
- Behaviour is focused on desired goals/outcomes
- People are motivated o perform behaviours that are valued (lead to rewards) and/or behaviours that they believe they can enact (self-efficacy)
- We learn what behaviours are rewarded, and how likely it is we can perform behaviour, from observing other
- Social learning is more likely to take place if the person is seen to be rewarded, is high status (e.g. a teacher, a medical consultant), is similar to use (e.g. colleagues, family) or friendly (e.g. friends).
- Modelling more effective if models high status or ‘like us’ (in terms of value/ ability). We are more likely to do something if it is valued by people we consider to be high-status or if the people are more like us in ability and valued by peers.
- This includes the negative influence of family, peers, media figures, and celebrities as role models which can lead us to harmful behaviours such as drinking, drug use.
- Positives: peer modeling/ education (e.g. safer sex) and celebrities in health promotion campaigns
What is the cognitive dissonance theory? (A Social Cognition model)
Cognitive dissonance theory (Festinger 1957)
- Discomfort when hold inconsistent beliefs or actions/events don’t match beliefs (inconsistent with reality or behaviours)
- Reduce discomfort by changing beliefs or behaviour
- Health promotion; providing health information (usually uncomfortable) creates mental discomfort and can prompt change in behaviour e.g. smoking kills signs on cigarette packets. BUT information alone is not effective.
- Also there is evidence that if you give people information that triggers fear, that can be counter-productive as it could lead to information avoidance.
Describe the Health Belief Model (Social Cognition Model No.2)
Health Belief Model (Becker 1974)
- Beliefs about health threat (perceived susceptibility and perceived severity) and beliefs about health-related behaviour (perceived benefits, perceived barriers) and cues to action (e.g. condom vending machines in toilets prompting you, education, symptoms, media) are all influences in making decisions about engaging in health behaviors.
- To use the HBM in clinical practice, we should explore patients’ perceived susceptibility, severity, benefits and barriers as well as any cues. People’s perceptions of threat and benefits can be improved through education. Problem solving and action plans could be used to reduce perceived barriers. Using HBM to design interventions has proved very effective. For example, Yabroff and Mandelblatt (1999) looked at 63 interventions designed to increase breast cancer screening through mammograms. Interventions based on the HBM were 23% more effective than the usual care.

What are the limitations of the health belief model?
Limitations of HBM:
[*] Rational and reasoned? Sex/chocolate
[*] Decisions? –habit/conditioned behaviour/ coercion
[*] Doesn’t recognize other factors such as Emotion factors (e.g. fear, desire)
[*] Incomplete (self-efficacy, broader social factors)
Explain about the theory of planned behaviour
We need to understand their intention first!
- What do I think about the planned behaviour? What do others think about the planned behaviour? What control do I have?
- Interventions based on the TPB appear to be effective. One recent, well-designed study used the TPB to develop a leaflet to encourage school children to exercise more. This study found that children who received the intervention reported changes in their attitude towards exercise, subjective norm, behavioural control and intentions. They were also more likely to have increased their exercise than children in the control group.
- Intention Behaviour Gap: good predictor of intentions but poor predictor of behaviour.
- The problem is translating intentions into behaviour
- Implementation intentions (Gollwitzer 1993): translating intentions into behaviour.
[*] Concrete plans of action – what will I do when and where. Writing down plans has been shown to be effective.
[*] E.g. volitional help sheet (writing if-then statements) (Armitage 2008)

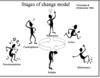
Describe a model of stages of behaviour change
Stages of Change (transtheoretical) model
- The way people think about health behaviours and willingness to change their behaviour are not static
- Stages of change model: 5 stages which people may pass through over time in decision making / change
- Different cognitions may be important determinants of health behaviour at different times.
- In precontemplation, a person is not even considering changing their behaviour. In contemplation they begin to consider changing. This leads into preparation where the individual prepares to change. The final two stages are action and maintenance where the person makes the change in the short term (action) and this behaviour change is consolidated and maintained in the long term (maintenance).
- Prochaska and DiClemente 1984
- Stages of change model describes process of change
- Support should be given at the contemplation stage.
What are the strengths of the transtheoretical model? In particular think about relapse
- Relapse is part of the cycle and common. Important for patient not to see relapse as failure. Patients may have to go through the cycle a few times before the new behaviour becomes permanent. The advantage of this is that it normalizes relapse and encourages people not to see this as a failure but to keep trying to change their behaviour. In clinical practice a healthcare professional could emphasize this and explore what a person has learned from a relapse and how this can be used to increase chances of success next time.
- The strengths of this model is that it recognizes people are at different stages of readiness for change and that interventions should be tailored to their particular stage. Another strength is the inclusion of relapse which is particularly important in addictive behaviour where relapse is common.
Why people might use drugs and alcohol?
- Pleasure
- Entertainment
- Social lubricant
- Enhance creativity
- Enhance other experiences like dancing, music, sex
- Peer influence
- Relieve boredom
- Relieve anxiety, depression, stress…
- Forget worries
- Relief from pain
- Spiritual quest
How should we consider context?
Context: substance + mind set + setting = consequences (Dr Norman Zinberg)
Social and Psychological Context:
- Cause: social, environmental, interpersonal factors, psychological, emotional and intrapersonal factors all can lead to Effect. It is a cycle not a linear relationship. E.g. going to prison -> taking drugs -> going to prison.
Social Context: people living in the more deprived areas are more likely to be frequent drug users (4.5%) compared with people living in the least deprived areas (2.3%). Clearly a medial or genetic model cannot adequately account for things.

What’s a rough estimate of the number of people in the UK with drug use problems? And rough cost to society?
A rough estimate is that about half a million people in the Uk experience problems with drug use. NB: the figures are estimates and subject to distortions.
‘problem drug use’ is not easy to define
And consider ‘iatrogenic’ problems: patient can become addicted to prescription drugs due to long term use
Cost of Drug Use is estimated £15 billion
£1 spent on treatment savies society £2.50
306,000 crack and heroin users in England (2012) but this figure is falling.
103,000 people inject drugs, this figure is falling
Deaths related to drugs in 2010 = 1784
What problems are alcohol misuse associated with?
Alcohol misuse is associated with a wide range of problems including physical health problems such as cancer and heart disease, offending behaviours such as domestic violence, suicide and deliberate self-harm, child abuse and child neglect and mental health problems which co-exist with alcohol misuse and social problems such as homelessness.
Total cost of alcohol related harm ~25 billion (to society)
- Cost t NHS; ~2.7 billion
- >8000 deaths directly related to alcohol
- >20,000 deaths indirectly related to alcohol
- >1 million Alcohol-related hospital admissions
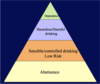
Define Low Risk Drinking
- Abstention: non-drinkers
- Low Risk Drinking: people who drink within the Department of Health’s sensible drinking guidelines and hence are at low risk of harmful effects
Define Hazardous Drinking
- people who are drinking over the sensible drinking limits, either in terms of regular excessive consumption or less frequent sessions of heavy drinking. However they have so far avoided significant alcohol-related problems.
- WHO Definition: a pattern of use that increases the risk of harmful consequences for the user…that are of public health significance despite the absence of any current disorder in the individual user
Define Harmful Drinking
- drinking at levels above those recommended for sensible drinking, typically at higher levels than most ‘hazardous drinkers. Harmful drinkers show clear evidence of some alcohol-related harm.
- Many harmful drinkers may not have understood the link between their drinking and the range of problems they may be experiencing.
- WHO Definition: a pattern of use, which is already causing damage to health. The damage may be physical or mental
Define Moderate Dependence
drinkers who have a ‘degree’ of dependence but who have not reached the stage of ‘relief drinking’ which is to say drinking to avoid physical discomfort from withdrawal symptoms. They could suitable for a detox in the community.
Define Severe Dependence
people may have serious and long standing problems “chronic alcoholics”
Typically they have experienced significant alcohol withdrawal and may have formed the habit of drinking to stop withdrawal symptoms
They may require an in-patient alcohol detox
Complex needs: this is an extension of the category of severely dependent drinkers.
- Drinkers with complex needs such as psychiatric problems, poly-drug dependence, homelessness and multiple previous episodes of treatment.