What are the two broad categories of Sexual problems
- Impairments to physiology ie: sexual dysfunction
- Impairments in the human relations part of the sexual experiance ie: diffiulties/consequences of the ways people conduct themselves sexually
What types of non-physiological sexual dysfunction is there?
Psychological:
- interpsychic- relationships, communication
- Intrapsychic- beliefs, meanings, conflicts, guilt, shame, information distortion, past sexual trauma, depression/anxiety
Social:
- Situational
Whats the PLISSIT model?
Developed as a solution for sexual counselling.
Suggests interventions for some common sexual dysfunctions.
4 levels of complexity:
Permission to talk about sexual matters, fantasize
Limited Information
Specific Suggestions
Intensive Therapy
Female Sexual Dysfunction
Sexual interest/aurosal disorder: low desire the most common complaint.
Female orgasmic disorder
Genito-pelvix pain/penetration disorder
- Must be 75-100% of the time
- minimum duration of ~6months
- cause significant stress
Lifelong vs acquired
Severity scale
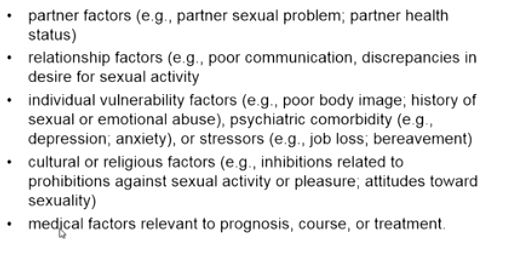
Associated factors of female sexual dysfunction
Treatment of FSD
Is there really a problem? Who’s problem is it?
Education
- *Counselling**:
- patient/couple
- sensate focus
Manage medical issues: menopause, hormone replacement therapy, physiotherapy
Male Sexual Dysfunction
- Male hypoactive sexual desire disorder
- Delayed ejaculation
- Erectile Disorder
- Premature ejaculation
***same associated factors as women
Low libido in men
- Psycholoical: fatigue, situational factors, depression
- Physical: hypothroidism, hypogonadism (low testosterone), PADAM
- Other: medication
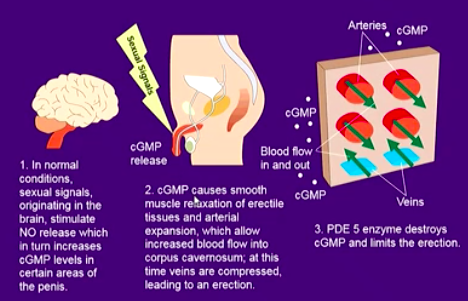
Biomedical mechanisms in getting an erection
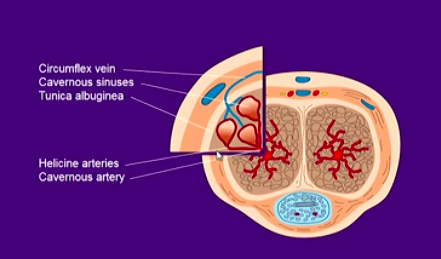
Anatomy of a flaccid penis
During erection these arteries (helecine and cavernossus) swell and compress the veins
Definition of Erectile Dysfunction
Persistant inability for at least 3 months, to obtain/maintaina n erection sufficient for satisfactory sexual performance
-Increases with age
Organic vs psychogenic
-Chronic illness, surgery, trauma
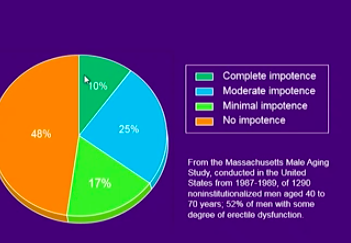
What percentage of men age 40-70yrs experiance ED?
~52%
only around 10% full impotence
What is the Cause of Erectile Dysfunction
Organic: vascular, neurological, hormonal issues
Psychogenic: usually secondary
- Can be a combo of both*
- Eg: systemic disease, neurogenic disease, penile dosorder, psychiatric dsorder, endocrine disorder*
Chronic Illness: a penile disorder example?
Peyronie’s disease: a fibrous change, a thickening in the tunica (from previous inflamm process) → physical distortion of the erect penis.
1/3 get better, 1/3 get worse, 1/3 stay the same
How can prostate surgery be an issue?
Can damage many vessels/nerves → erectile dysfunction
What types of surgery can lead to erectile dysfunction?
Spinal cord injury
Pelvic injury/surgery
Prostatectomy
Modifiable factors of Erectile Dysfunction
- Alcohol consumption
- Cigarette smoking
- Drugs: anti-hypertensives, anti-depressants, hormones, tranquelizers etc
These can be controlled by the patient!
Basic Management of ED
Diagnose the issue
Evaluate co-morbidities: heart disease, vascular disease, depression
What does the couple want?
Adjust meds
Address lifestyle
Education
Tailored treatment
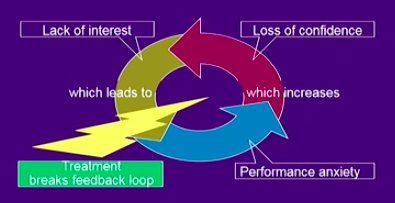
Why/how is a lot ofthe psygoneic issues secondary?
Something goes wrong → loss of confidence →lack of interest → performance anxiety → sexual dysfunction/ actual issues during the sexual experiance
Treatment for performance anxiety and ED
Mindfulness based approach a component
Non-invasive options for Erectile Dysfunction treatment
- eliminate modifiable risk factors
- Counselling and/or psychotherapy
- medication
- vacuum constriction devices
Invasive therapy trreatments for ED
- Transurethtral drug application
- Intracavernous injection therapy
- Prosthesis implantation
- Venous/arterial surgery
Phosphodiestarase 5 inhibitors (PDE5) used are?
- Sildenafil: ‘viagra’
- Tadalafil: ‘Cialis’ longer duration of action, option of low dose (5mg) daily, (maintains oxygenation thus improving endothelial smooth muscle health)
- Vardenafil: ‘Levitra’, shorter duration of action
Other drug/physical approaches to ED treatment?
- Alprostadil injected into c.cavernosa
- Bimix
- Trimix
- ED shock wave theray
- Vacuum device
- Surgery
These can lead onto other issues!
-
Renal Histology24
-
Renal Phys: Body Fluid Comp PART 112
-
Renal Phys: Body Fluid comp PART 218
-
Glom and Tubular Function 131
-
Glom and Tubular Function 225
-
Kidneys, Ureter, Bladder and Posterior Abdominal Wall38
-
Clinical Renal Failure and tests32
-
Haematuria Proteinuria31
-
Inguinal Canal and Spermatic Cord21
-
Radiology Imaging of the Renal Tract14
-
Imaging the Female and Male Pelvis0
-
Child Birth27
-
Integration of Salt and Water Balance14
-
Pelvic Contents27
-
Perineum23
-
Acid-base Balance #119
-
Acid-Base Balance #217
-
Integration of Salt and water Balance 216
-
Clinical Problems: Kidney Failure20
-
Clinical Problems: Electrolytes23
-
Clinical Gynaecology22
-
Male and female Genitalia27
-
Testes and Penis pathology23
-
Carcinoma of the prostate18
-
Sexual Function and Dysfunction30
-
Pathology of the ovary and uterus0
-
Cervical screening and pathology31
-
Sexually Transmitted Diseases27
