What is the likely diagnosis?
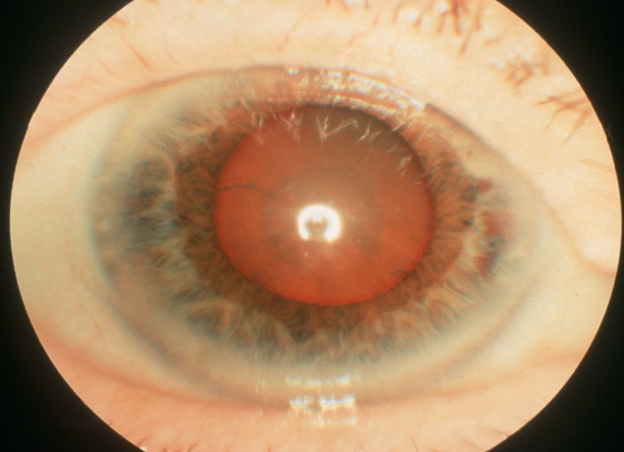
Defective red reflex → sign of cataracts
What would you do initially (examination) in a patient presenting with a possible squint?
- pen torch → examination of red light reflex from two eyes
(Is it symmetrical? Cover the eye that appears to be looking at the light. Does the other (uncovered) eye move to look at the pen torch?)
- ophthalmoscope → check to see if there is a red reflex in both eyes.
What does this photograph show and what would you do next? What is the commonest cause of this condition?

This is a convergent squint (strabismus) (esotropia)
- most commonly due to a refractive error (hypermetropia, hyperopia, long sightedness)
- Refer to the Eye Clinic
What happens to the sight if the squint persists?
The eye becomes ‘lazy’ (amblyopic)
What does this photo show?
What to do next?
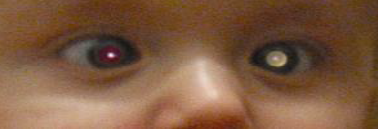
- Loss of the red reflex (possible retinoblastoma)
- Phone or fax the eye clinic for an URGENT opinion
What eye conditions (in the elderly) may contribute to falls and difficulty in reading?
Examples
- Cataract
- ARMD
- Glaucoma
- A CVA affecting the field of vision
(3) initial assessment in a patient presenting with loss of vision?
- Measure the visual acuity
- Test the field of vision to confrontation
- ophthalmoscopy
What are the initial management steps for a patient presenting with cataracts? (3)
- an optometrist → glasses will possible improve her vision
- the optician → to see if there might be anything else causing her sight difficulties
- referral to an ophthalmologist → possible surgery
Hx: am 70 years old. Yesterday I couldn’t see out of my left eye. It came on quite quickly and lasted about 15 minutes. Then it slowly recovered. It happened last week as well.
What do you want to ask about?
Was there any:
- headache (giant arthritis)
- jaw claudication (giant arthritis)
- difficulty combing the hair? (Giant cell arteritis)
- any risk factors for a stroke (CVA)?
Hx: I am 70 years old. Yesterday I couldn’t see out of my left eye. It came on quite quickly and lasted about 15 minutes. Then it slowly recovered. It happened last week as well. + headache (L sided)
What would you do? (initial examinations)
- Measure the visual acuity and test the fields to confrontation
- Check the BP and pulse rate / rhythm, listen to the neck with a stethoscope
- Feel for the superficial temporal arteries
- Organise an ESR and CRP measurement
- Consider urgent therapy and review (e.g. Aspirin if TIA, Prednisolone if temporal arthritis)
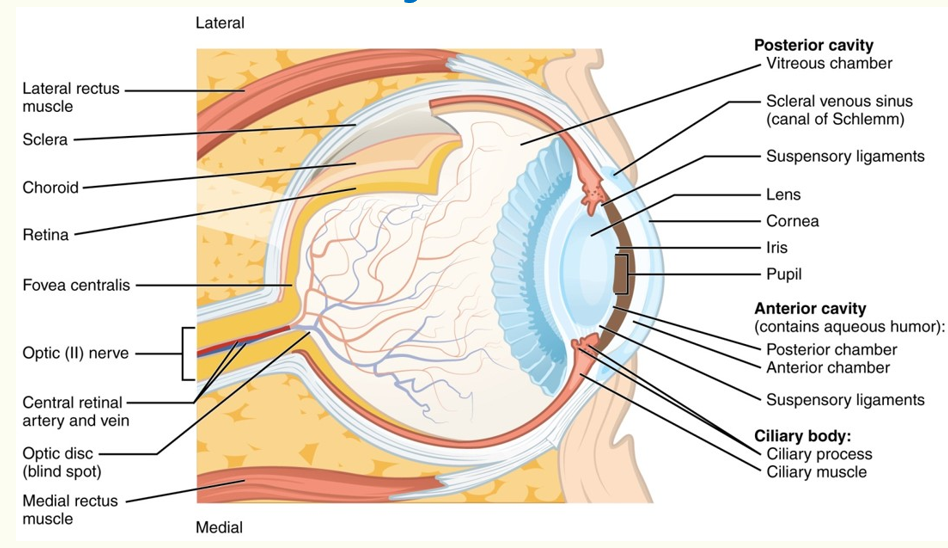
Eye anatomy - draw a diagram + label
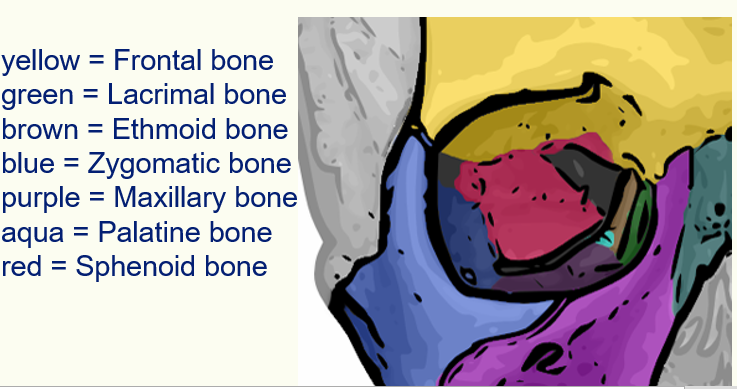
Name these coloured bones

Draw and label/name extraocular muscles
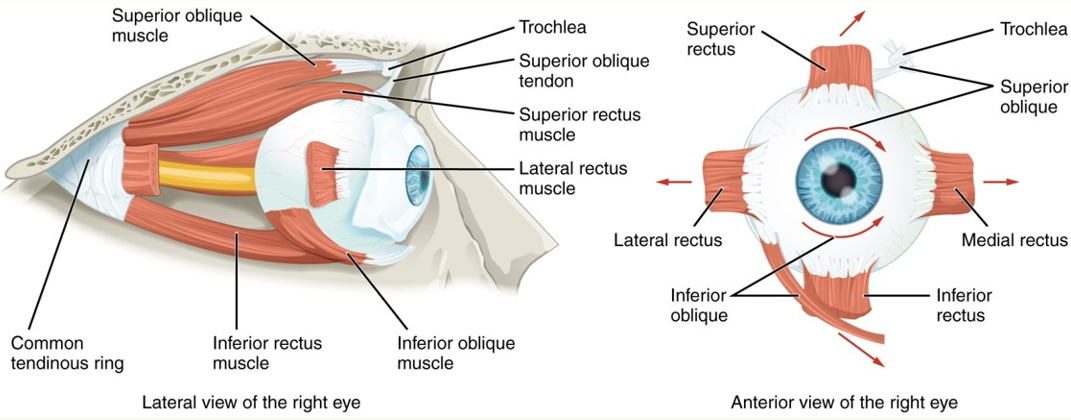
What cranial nerves supply which extraocular muscles?
IV Trochlear → superior oblique
VI Abducens → lateral rectus
III oculomotor → the rest and + levator and pupillary constriction
What pattern of visual defect is that?

Bitemporal hemianopia
What attern of visual defect is that?

Left homonymous hemianopia
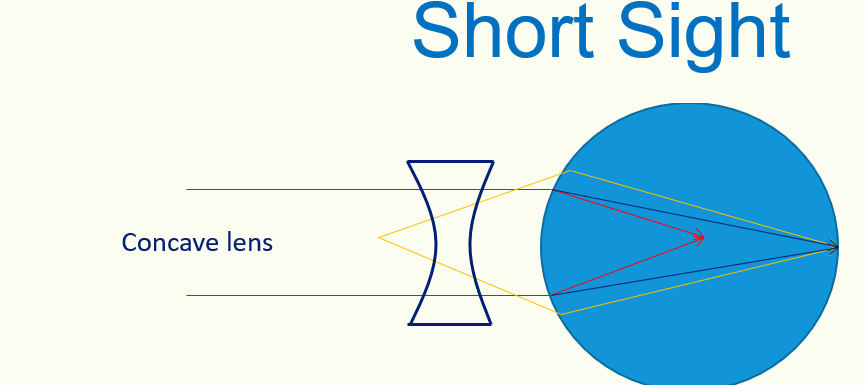
Type of lens used to treat short-sightedness
Concave lens
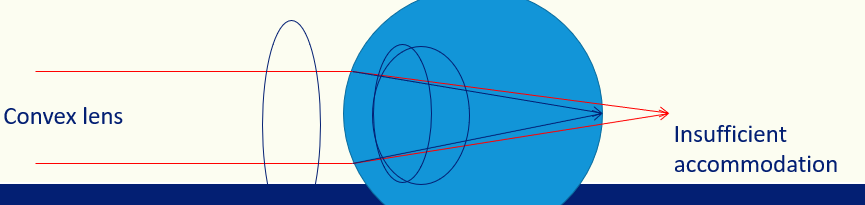
Types of lens used to treat long-sightedness
Convex lens
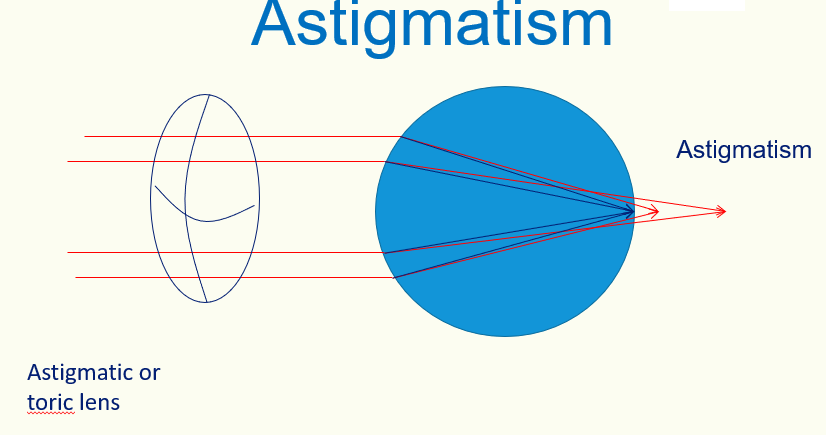
Type of lens used to treat Astigmatism
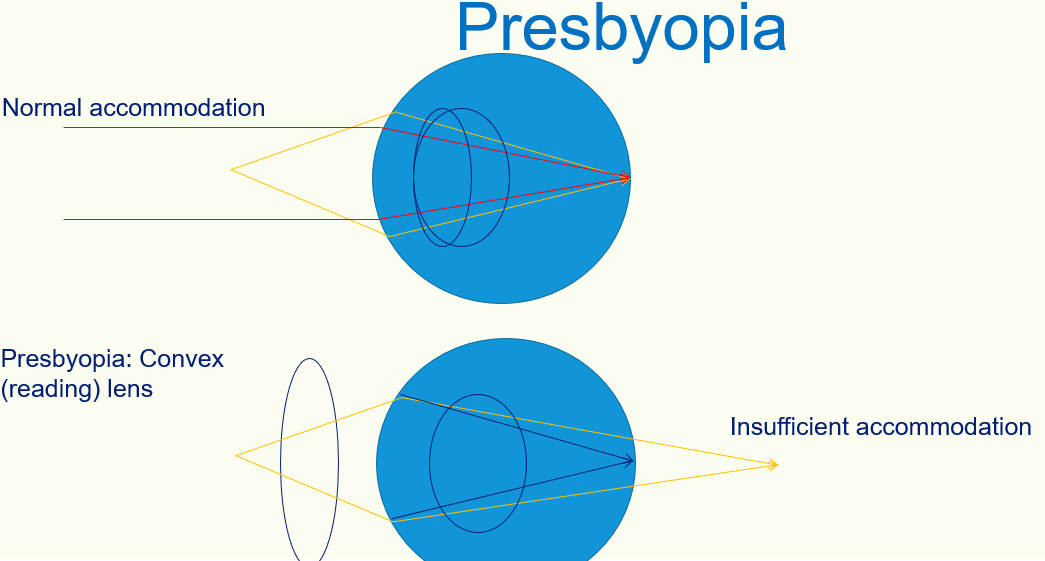
Type of lens used to treat Presbyopia
4 main causes of visual loss in the elderly
- cataracts
- age-related macular degeneration
- diabetic retinopathy
- glaucoma
4 main causes of visual loss in adult (not the elderly)
- refractive error
- keratoconus (thinning of cornea →cone-like shape develops)
- familial
- childhood eye disorder
4 main causes of visual loss in children
- strabismus
- refractive error
- leucocoria = white pupilary reflex (sign of number of conditions: retinoblastoma, congenital cataracts, corneal scarring, melanoma)
- rare retinal disease
Main causes of rapid onset visual loss
- retinal artery or vein occlusion
- retinal detachment
- wet ARMD
- neuritis
- ischaemia (including arteritis)


















-
Surgery: Opthalmology74
-
Surgery: Upper Limb (Orthopedics)72
-
Surgery: Benign Breast Disease61
-
Surgery: Breast Cancer45
-
Surgery: ENT95
-
Surgery: Lower Limb (orthopedics)55
-
Surgery: Ortho_extra notes19
-
Surgery: BPH and Prostate Cancer57
-
Surgery: Scrotal lumps61
-
Medicine: AKI and CKD47
-
Medicine: Imaging and investigations22
-
Medicine: Restrictive lung diseases, Pulmonary hypertension and O2 therapy30
-
Medicine: ECG interpreatation35
-
Medicine: Cerebrovascular disease37
-
Medicine: VTE48
-
Obs&Gyn: Infertility40
-
Obs&Gyn: Gyn malignancies45
-
Obs&gyn: Obesity42
-
Obs&Gyn Urinary incontinence36
-
Paeds: Mental Health (1)35
-
Paeds: Mental Health (2)28
-
Paeds: Endocrinology (1)30
-
Paeds: Endocrinology (2)35
-
Mental Health: Schizophrenia (1)56
-
Paeds: The Limping Child (1)30
-
Paeds: The Limping Child (2)32
-
Paeds: The Limping Child (3)30
-
Mental Health: depression34
-
Mental Heatlh: Mental Health Act40
-
Peads: Diabetes in children45
-
Mental Health: Substance Abuse65
-
Radiology 130
