Week 3 Flashcards
(77 cards)
Define the Yerkes-Dodson Law and describe the relationships between stress, performance, and learning
Performance adn adaptive learning areoptimal under moderate rather than either high or low stress
Describe the roles of the amygdala and hippocampus in the fight or flight response
Modeate stress conditions activate the limbic system, facilitating the coordinated ability of the amygdala, hippocampus, and prefrontal cortex to analyze, respond to , and learn from the challenge.
amygdala coordinates an emergent reaction arousing and mobilizing the organism bia the sympatho-adrenomedullary (SAM)
hypothalamus leads to release of catecholamines and glucocorticoids
Summarize the role of glucocorticoids play in the regulation of the stress response
Glucocorticoids
CRH -> ACTH & Beta endorphin -> Glucocorticoids
Can inhibit protein synthesis
Accelerate protein catabloism
Increase lipolysis
Decrease peripheral glucose utilization
Bone loss
Muscle wasting
Immune system suppression
Describe what evolutionary objective most illnesses seen in primary care are the by-product of
Surivival of the organism and the survival of the species
Summarize the ways in which chronic stress affects metabolic processes, growth processes, and reproductive processes
Shunting of stored nutrients to muscle
Shutting down of digestion and other non-essential functions
Inability to respond to insulin (metabolic syndrome)
Impairs normal growth and development via sympathic NS, inhibited growth hormone, and shortening of telomeres
High levels of stress may result in glucocorticoid inhibiton of hypothalamic release of lutenizing hormone (LH) and follicle stimulating hormone (FSH). Sperm and egg production inhibition.
Explain the bio-behavioral mechanisms by which stress contributes to immune system disorders
Acute/moderate stress generally activates the genetically programmed immune system
Excess of glucocorticoids (chronic stress) may impair production of B cells and T cells. Premature migration of T cells to thymus resulting in its shrikage
Impari NK
Heighten immune system response when body is attacked and can lead to autoimmune disorders
Explain the bio-behavioral mechanisms by which stress contributes to cardiovascular disorders
High stress diminishes arterial flow increasing blood pressure
Decrease urine
Artheriosclerosis
List the disorders associated with chronic stress-induced system failures
anticipatory anxiety (fear)
depression
learned helplessness
PTSD due to helplessness and powerlessness
Define the Holmes and Rahe scale and describe the relationship between life units and illness
Attemptes to quantify the relative importance of life changes in terms of distress of the individual
Exercise and stress
Mindfullness and stress
Moderate exercise -> Longer telomeres (too much shortens)
Mindfullness -> genes associated with telomeres, insluin, and metabloism
Distinguish between adaptive and maladaptive strategies for coping with stress and research
Direct action (preparation, assertive, practive, mastery)
Avoidance (withdrawal/sleeping, denial, rationalization, substance abuse)
Palliation (exercise)
Summarize the role of the unconscious in motivation, according to psychodynamic theory
Behavior is motivated by unconscious biological urges, instincts, or drives
Where is the blood flowing the most?
Where is the blood flowing the most if normalized per mass?
At rest where is 50% of blood flowing?
Which organtake up 5% of CO, but accounts for 10% of oxygen conusumption
Liver / kidney muscle
Kideny / heart
Liver / kideny
heart

“Ohm’s Law” - blood flow
Puiseulle’s Law
Q = dP/R
R=8nl / (PI*r4)
Q = dP r4 PI / 8 n l
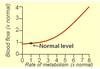
Relationship between metabolsi and blood flow
Proportional
Blood flow regulated to satisfy minimum requirements of tissue
When blood flow is regulated what variables can be altered?
CO
Resistance
Capacitance of veins
Extracellular fluid volume and osmolality
Where can the control of blood flow come from?
Local (intrinsic) mechanisms
Systemic (extrinsic) mechanisms
Types of local control of blood flow and examples
Types of systemic control of blood flow and examples
Intrinsic
Metabolic: release of vasodilators, nutrient deficiency for vascular smooth muscle
Myogenic: sudden strech, reduced strech
Systemic
Humoral: adrenal hormones, Renin-angiotensin-aldosterone system (RAAS), endothelins, kinins, natriuretic peptides
Neural: Sympathetic, parasympathetic
Pressure Flow Autoregulation
Local or systemic?
When fails?
Local control
Constant flow under varying pressures (strech activated Ca2+ channels)
At high pressures resistance cannot be appreciable further decresed.
The changes in blood flow in response to overall homeostasisare not classified as autoregulatory processes.

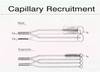
Hyperemia (increased blood flow)
What is active active hyperemia?
What is reactive hyperemia?
Possible causes?
Active hyperemia is increased blood flow caused by increased tissue activity
Reactive Hyperemia is blood flow above control level upon release of an arterial occlusion
Causes:
Deficiency of O2 (vasodilator release / inhibition of contraction)
Increased metabolism (vasodilator release / inhibition of contraction)
Endothelium-derived relaxing factor (EDRF)
It is produced and released by the endothelium to promote smooth muscle relaxation.
The best-characterized is nitric oxide (NO)
Different mechanisms that can activate production of NO in endothelial cells
iNOS = inducible nitric oxide synthase
cNOS = constitutive nitric oxide synthase

What hormones and their proportions that are released from Adrenal Medulla?
What is tumor associated with Adrenal medulla?
80% epinephrine and 20% norepinephrine
phenochromocytoma
Endothelins
Effect on heart?
Effect on hormones?
Effect on autonimic nervous system?
Effect on lungs?
Effect on kideny?
Vasoconstriction
Positive inotropic and chronotropic effect
Increase plasma levels of ANP, renin, aldosterone, and catecholamines
Increase release of sympathetic transmitters
Produce bronchoconstriction
Decrease glomerular filtration rate, renal blood flow, increases Na+ reabsorption