UW3 Flashcards
Question

B. Hyperfunctioning Pancreas
qualitative-qualitative
Chi-square
Logisitic Regression
qualitative-quantitative
T-test
ANOVA
Linear Regression
Quantitative-Qualitative
Logistic Regression
Quantitative-Quantitative
Correlation
Linear Regression
Anaphylaxis useful marker
Tryptase is pretty specific to mast cells and can be used as a marker for mast cell degranulation
Newborn hemodynamic changes
Immediately after birth, decreased pulmonary vascular resistance (due to oxygenation and ventilation of the lungs) and increased systemic vascular resistance (due to removal of the placenta from circulation) reverse the flow across the ductus arteriosus to left-to-right. Because the right ventricle no longer contributes to systemic blood flow, the left ventricle becomes responsible for the total cardiac output.
question

C. Observer bias
Observer bias (also known as expectancy bias) occurs when investigators misclassify data due to preconceived expectations or prior knowledge concerning the study or its participants. This type of bias is particularly important when outcomes are subjective (ie, involve personal interpretation of clinical, microscopic, or radiographic findings).
In this case, the pathologists who work at the hospital where the study is being conducted may know that the study is investigating diabetic nephropathy, or they may have access to additional medical records that indicate diabetes status. Conversely, the pathologists at other institutions are more likely to be blinded to the study’s objectives and the patients’ medical history.
Question

C. Ghrelin
The 24-hour hormone levels in the control subjects show increasing secretion leading up to meals, followed by a sharp postprandial drop. However, the subjects who have undergone gastrectomy show lower baseline levels with attenuation of meal-related fluctuations. This pattern suggests that the hormone is likely secreted in the stomach and suppressed by food intake, which is consistent with the secretory pattern of ghrelin.
Ghrelin is produced primarily in the stomach in response to fasting; levels surge leading up to meals and fall after eating. Ghrelin stimulates appetite and promotes weight gain. Caloric restriction and falling fat stores lead to increased ghrelin levels (along with decreased leptin and insulin levels), which limits weight loss from dietary modification alone. However, patients who have undergone bariatric procedures that remove a portion of the stomach (eg, roux-en-Y gastric bypass, sleeve gastrectomy) can lose a significant number of ghrelin-secreting cells. This leads to lower ghrelin levels and less stimulation of appetite in response to fasting, promoting weight loss.
Hunger and satiety control

Question

A. 5 alpha-reductase
Sexual development is influenced predominantly by 3 steroid hormones:
Testosterone: development of internal male genitalia (except prostate), spermatogenesis, male sexual differentiation at puberty (eg, muscle mass, libido)
Dihydrotestosterone (DHT): development of external male genitalia, growth of prostate, male-pattern hair growth; also amplifies effects of testosterone due to high affinity for testosterone receptor
Estrogen: endometrial proliferation, development of ovarian granulosa cells, breast development
5α-reductase converts testosterone to DHT. There are 2 types of 5α-reductase: type 1 is present in postpubescent skin, whereas type 2 is found predominantly in the genitals.
5α-reductase type 2 deficiency results in diminished conversion of testosterone to DHT in the male urogenital tract. In the phenotypically (46,XY) male fetus with this genetic defect, the internal genitalia (ie, testes) develop normally under the influence of testosterone. However, due to the lack of DHT, the testicles remain undescended (cryptorchid testes presenting as inguinal masses) and the external genitalia do not develop properly, ranging from a small phallus with hypospadias to ambiguous or female-type genitalia.
Testosterone levels are within the normal range because of intact negative feedback. At puberty, physiologic increased levels of testosterone and the action of 5α-reductase type 1 result in masculinization with male-pattern muscle mass, voice deepening, penile and scrotal growth, and testicular descent.
Mechanism of ovary development from undifferentiated gonad

Mechanism of testis development from undifferentiated gonad

Question

H. Mycoplasma pneumoniae
Mycoplasma pneumoniae infection is common in adolescents and usually presents with tracheobronchitis or walking pneumonia. The pathogen attaches to the respiratory epithelium using surface antigens (I-antigen) that are also present on the plasma membrane of erythrocytes. Therefore, patients with M pneumoniae typically develop cross-reactive IgM antibodies that can attach to red blood cells, activate the complement system, and cause erythrocyte lysis. These cross-reacting antibodies are called cold agglutinins because they bind to erythrocytes most strongly at temperatures below core body temperature. Testing for cold agglutinins can be done at the bedside by drawing blood into an edetate disodium–containing tube and placing it in a cup of ice. Removing the tube after several seconds will reveal clumping/agglutination that resolves as the tube warms.
Cold agglutinins are often asymptomatic, but some patients develop mild intravascular hemolytic anemia that usually resolves after 6-8 weeks (when IgM antibody titers fall). Patients who have infectious mononucleosis and certain hematologic malignancies also commonly develop cold agglutinins.
Educational objective:
Infection with Mycoplasma pneumoniae can result in the formation of cold agglutinins, which are IgM antibodies (primarily) that bind red blood cells and cause clumping/agglutinations at low body temperatures. Other illnesses resulting in cold agglutinin formation include infectious mononucleosis and certain hematologic malignancies.
Cold Agglutinin Disease

Warm Agglutinin Disease
SLE Systemic lupus erthematosis , CLL chronic lymphocytic Leukemia

Question

D. Increased 2, 3 BPG synthesis

This patient is most likely suffering from acute mountain sickness (AMS), a type of high-altitude illness resulting from low partial pressure of oxygen (pO2) in environments >2,500 m (8,000 ft). Although the fraction of oxygen in inspired air remains constant (21%) at different terrestrial elevations, barometric pressure drops with increasing altitude, leading to decreased pO2 in the air and lungs.
In an otherwise healthy patient, the pO2 rapidly equilibrates between the alveoli and arterial blood, causing hypoxemia when the pO2 drops below 80 mm Hg. Several acute physiological changes occur in response to the resulting hypobaric hypoxia:
Increased firing of peripheral chemoreceptors causes hyperventilation, which directly reduces hypoxemia and improves tissue oxygenation (Choice A).
Increased 2,3-bisphosphoglycerate (2,3-BPG) synthesis by erythrocytes, which shifts the O2-hemoglobin dissociation curve to the right, decreasing the affinity of hemoglobin for oxygen and facilitating the offloading of oxygen in peripheral tissues.
Hyperventilation also decreases the partial pressure of carbon dioxide, resulting in increased blood pH (respiratory alkalosis). Common symptoms of AMS include headache, fatigue, dyspnea, dizziness, and sleep disturbances. Most cases subside within 2 days but can progress to life-threatening cerebral and/or pulmonary edema in susceptible patients. In the absence of underlying pathology, symptoms typically resolve within 48 hours as the kidneys increase HCO3− excretion to compensate for the alkalosis, restoring pH toward the normal range and improving symptoms
Baroreceptors location and name
bodies are chemoreceptors
sinus and arch are baroreceptors

Blood Chemoreceptors location and names
Bodies are chemoreceptors
Sinus and arch are baroreceptors

Carotid body and sinus innervation
Glossopharyngeal Nerve

Aortic body and arch innervation
Vagus Nerve

Question

E. Sub Thalamic Nucleus

The subthalamic nucleus is a lens-shaped structure located ventral (inferior) to the thalamus, dorsal (superior) to the substantia nigra, and medial to the internal capsule. It is a component of the basal ganglia and plays an important role in the modulation of basal ganglia output.
Damage to the subthalamic nucleus can decrease excitation of the globus pallidus internus, thereby reducing inhibition of the thalamus. This may result in contralateral hemiballism, a movement disorder characterized by wild, involuntary, large-amplitude, flinging movements involving the proximal limbs (eg, arm and/or leg) on one side of the body. This most commonly occurs in the setting of lacunar stroke, which is often a consequence of long-standing hypertension and diabetes mellitus.
Basal Ganglia pathway

Posterior column pathway

Question

C. Masseter
This patient has jaw pain, a clicking noise when she chews, and associated headaches and neck stiffness, which is suggestive of temporomandibular joint (TMJ) syndrome. The underlying etiology of TMJ syndrome is multifactorial and includes TMJ derangement (eg, jaw misalignment, trauma), and hypersensitivity of the mandibular nerve (CN V3). Mechanical derangement of the TMJ can result in irritation and hypersensitivity of CN V3, leading to pathologic contraction of the masseter and pterygoid muscles (which worsens jaw pain and dysfunction). Spasms of these muscles can sometimes be palpated along the mandibular ramus.
Repetitive jaw motions (eg, gum chewing, teeth grinding) are thought to contribute to the development of TMJ syndrome due to increased workload and strain on the joint. Similar to some other musculoskeletal pain disorders (eg, tension headache), TMJ pain also seems to be related to psychiatric conditions and emotional distress.
question

C. Infection with a different viral serotype

This patient recently traveled to South America and now has several manifestations of dengue, a Flavivirus infection transmitted by female Aedes mosquitoes. Although primary (first) infections can be asymptomatic, adult patients may develop high fever, retroorbital pain, and severe myalgia/arthralgia, which gives dengue its common name breakbone fever. Hemorrhagic symptoms (eg, epistaxis, petechiae/purpura) can also occur, and laboratory evaluation often shows leukopenia, thrombocytopenia, and elevated transaminases. Most primary infections resolve spontaneously within 3-5 days and lead to lifelong protective immunity against the infecting viral serotype.
However, there are 4 dengue virus serotypes, and secondary infection with a different viral serotype is common and is usually associated with more severe illness. Secondary infections are particularly likely to cause dengue shock syndrome, a life-threatening dysregulation marked by increased capillary permeability, circulatory collapse (eg, shock), and end-organ damage (eg, stupor).
Although the exact pathogenesis of dengue shock syndrome remains unclear, it is probably due to the formation of nonneutralizing, cross-reactive antibodies during primary infection that then trigger antibody-dependent enhancement of secondary infection. There may also be accelerated (not blunted) T-lymphocyte activity against secondary infection due to display of cross-reacting viral antigens on major histocompatibility complexes of infected cells
Question

A. Chlorpheniramine
Diazepam is a long-acting benzodiazepine indicated as follows:
As an anxiolytic, it is effective for the management of generalized anxiety disorder and panic attacks.
The sedative-hypnotic effect of diazepam is useful for the short-term treatment of insomnia.
As an anticonvulsant, diazepam is indicated for status epilepticus. It is a first-line agent (along with chlordiazepoxide) for the treatment of seizures associated with alcohol withdrawal.
As a muscle relaxant, diazepam can stop the spasticity caused by upper motor neuron disorders (multiple sclerosis, strokes, spinal cord trauma) and tetanus.
The most common side effect of diazepam is sedation. Diazepam may also impair coordination and balance (sometimes avoided in the elderly for fear of falls), decrease memory and concentration, and produce confusion. These effects are amplified by the coadministration of other CNS-depressants. As a class, all benzodiazepines should be excluded from use in conjunction with alcohol, barbiturates, neuroleptics, or first-generation antihistamines.
Among drugs listed in the answer choices, only chlorpheniramine causes sedation and should not be used with diazepam. Chlorpheniramine is a first-generation antihistamine that acts by blocking both central and peripheral H1 receptors. Chlorpheniramine and other first-generation antihistamines can be very sedating because they easily penetrate the blood-brain barrier and accumulate in the CNS. The most sedating of this generation of antihistamines are diphenhydramine, promethazine, and hydroxyzine. Despite the associated sedation, these antihistamines are often still used to prevent/treat allergic reactions and motion sickness and as antiemetics.
Question

B. Glutathione Reductase

This patient likely has glucose-6-phosphate dehydrogenase (G6PD) deficiency, an X-linked recessive disorder causing hemolytic anemia and jaundice in response to oxidant stressors (eg, sulfonamide & antimalarial drugs, infection). Heinz bodies (oxidized hemoglobin conglomerates) precipitate in red blood cells and are removed by splenic macrophages, leaving behind characteristic bite cells.
G6PD is an enzyme of the pentose phosphate pathway. It generates the reducing agent NADPH, which is essential for detoxification of hydrogen peroxide produced by partial reduction of molecular oxygen in red blood cells. In the absence of NADPH, reduced glutathione (the molecule required for reduction of hydrogen peroxide to water) remains in an oxidized state, and red blood cells become susceptible to oxidative damage.
Glutathione reductase catalyzes the reduction of oxidized glutathione. Its absence leads to an inability to use NADPH to reduce glutathione, resulting in a clinical scenario similar to G6PD deficiency.
Features of G6PD
glucose-6-phosphate dehydrogenase (G6PD) deficiency, an X-linked recessive disorder causing hemolytic anemia and jaundice in response to oxidant stressors (eg, sulfonamide & antimalarial drugs, infection). Heinz bodies (oxidized hemoglobin conglomerates) precipitate in red blood cells and are removed by splenic macrophages, leaving behind characteristic bite cells.
G6PD is an enzyme of the pentose phosphate pathway. It generates the reducing agent NADPH, which is essential for detoxification of hydrogen peroxide produced by partial reduction of molecular oxygen in red blood cells. In the absence of NADPH, reduced glutathione (the molecule required for reduction of hydrogen peroxide to water) remains in an oxidized state, and red blood cells become susceptible to oxidative damage.

Question

C. Trigeminal

This patient’s presentation is most consistent with temporomandibular joint disorder (TMD). The underlying etiology of TMD is multifactorial and includes temporomandibular joint derangement (eg, jaw misalignment, jaw clenching/teeth grinding, trauma) and hypersensitivity of the mandibular nerve (CN V3). In addition to the classic symptoms of dull, waxing-and-waning face/jaw pain (worse with chewing) and clicking/popping noises with jaw movement, TMD can also present with ear-related symptoms (eg, ear pain, ear stuffiness, tinnitus).
Many of these clinical findings are due to involvement of the mandibular nerve (CN V3), which is the largest branch of the trigeminal nerve. It supplies sensation to the temporomandibular joint, floor of mouth, anterior tongue, and lower part of the face. In addition, it contributes to the sensory innervation of the external auditory canal; therefore, TMD can present with ear pain that is referred from the jaw joint. Ear stuffiness may be related to hypersensitivity affecting the tensor tympani. Theories regarding tinnitus in TMD include the proximity of the muscles of mastication to the ear and central connections between nerve supply of the temporomandibular joint and the areas of the brain involved in hearing.
Question

A. Gastric Antrum

Peptic (eg, duodenal, gastric, gastroesophageal) ulcers are most commonly due to Helicobacter pylori infection or use of nonsteroidal anti-inflammatory drugs. Because this patient takes no medications, his ulcer is likely due to H pylori infection. The site of ulcer formation is dependent on relative bacterial colonization density within the stomach. H pylori preferentially colonizes the gastric antrum, particularly early in the disease, although it may occur in other areas of the stomach or spread with time.
Colonization of H pylori in the gastric antrum is associated with decreased somatostatin formation and increased gastrin secretion, which stimulate the parietal cells to produce excess acid. This results in an increased acid load emptying into the proximal duodenum, leading to duodenal ulcer (DU) formation. Biopsy of the antrum can confirm H pylori infection in patients with a DU, which characteristically presents with upper abdominal pain that improves with eating.
In contrast, gastric ulcers (GUs) are associated with colonization in the gastric corpus (body). The etiology of GUs is not acid related, as these patients typically have normal or reduced acid levels, but is thought to be due to direct mucosal damage and chronic inflammation. Unlike DU pain, GU pain often worsens with eating.
Question

C. Granulomatous …
This patient with hilar lymphadenopathy, nodular pulmonary infiltrates, and a history of anterior uveitis likely has sarcoidosis, an inflammatory disorder of unknown etiology that occurs most commonly in younger, African American patients. It is characterized on histology by the presence of noncaseating granulomas (collections of tightly clustered, epithelioid macrophages with abundant pink cytoplasm surrounded by a rim of mononuclear cells without central necrosis). Multinucleated giant cells, formed by macrophage fusion, are frequently seen.
Sarcoidosis primarily involves the lungs, causing nodular or interstitial infiltrates. However, extrapulmonary manifestations are common and can involve the lymph nodes (eg, hilar adenopathy), eyes (eg, anterior uveitis), skin (eg, erythematous nodular rashes), CNS (eg, neurosarcoidosis), and internal organs (eg, heart, liver). Salivary glands (eg, parotid, as in this patient) are involved in up to 5% of patients. Constitutional symptoms, including fatigue, weight loss, and night sweats, can also occur.
Question

C. Kawasaki Disease
This patient has Kawasaki disease, an acute, inflammatory condition characterized by vasculitis of medium-sized arteries. Most cases occur in children age <5 with a peak incidence among those of East Asian ethnicity. The persistent release of proinflammatory cytokines causes irritability and a prolonged high fever that is often unresponsive to antipyretics.
Diagnosis is clinical, consisting of fever ≥5 days and ≥4 of the following findings:
Conjunctivitis: bilateral, nonexudative, limbus sparing
Mucositis: erythematous, fissured lips; strawberry tongue
Rash: polymorphous, often begins in perineal area
Distal extremity changes: erythema, edema, desquamation of the hands and feet
Cervical lymphadenopathy
A serious complication of Kawasaki disease is coronary artery inflammation leading to the development of coronary artery aneurysms, which can lead to myocardial ischemia, arrhythmias, and sudden death.

Kawasaki Disease Features
prolonged high fever that is often unresponsive to antipyretics.
Diagnosis is clinical, consisting of fever ≥5 days and ≥4 of the following findings:
Conjunctivitis: bilateral, nonexudative, limbus sparing
Mucositis: erythematous, fissured lips; strawberry tongue
Rash: polymorphous, often begins in perineal area
Distal extremity changes: erythema, edema, desquamation of the hands and feet
Cervical lymphadenopathy

Question

A. Acquired von willebrand deficiency

This patient with severe aortic stenosis (AS) has symptomatic anemia (dyspnea, fatigue) with low mean corpuscular volume likely due to chronic bleeding from colonic angiodysplasias. Colonic, mucosal, and cutaneous bleeding is common in patients with severe AS due to acquired von Willebrand syndrome.
Von Willebrand factor (vWF) is a multimeric glycoprotein generated by endothelial cells and platelets. It plays 3 important roles in hemostasis:
vWF binds to sites of endothelial injury and serves as a scaffold for platelet aggregation.
vWF promotes platelet aggregation at sites of high shearing pressure (often seen in areas of endothelial injury).
vWF acts as a carrier protein for factor VIII, which dramatically reduces the metabolism of factor VIII.
The activity of vWF is greatest when it is in large, multimeric forms. However, large multimers of vWF are also most susceptible to unfolding in areas of high shear forces, exposing a cleavage site that makes them more vulnerable to destruction by the ADAMTS13 metalloproteinase. Because patients with severe AS typically have high shearing forces across the damaged valve, they have increased cleavage of vWF multimers, which eventually leads to vWF deficiency. Valve repair can reverse the bleeding diathesis.
Question

E. Tyrosinase

This patient’s eye findings and white hair are consistent with oculocutaneous albinism (OCA), an autosomal recessive disorder of melanin production or distribution. The most common defect is in the enzyme tyrosinase, which converts tyrosine to DOPA in the first step of the melanin biosynthetic pathway.
Melanin is produced in melanosomes (specialized organelles within melanocytes), which are then transferred to keratinocytes to provide ultraviolet protection. In patients with OCA, lack of this pigment results in the characteristic white hair and skin and translucent, light-colored irides. Iris transillumination occurs due to the reflection of light off the retina, causing the iris to appear red. Because the translucent irides allow in excess light, patients often have photophobia (light sensitivity).
In addition to pigmentation, melanin plays a role in guiding embryologic development of ocular structures. Without melanin, patients have misrouted and underdeveloped optic nerve fibers and hypoplastic or absent foveae, as seen in this infant. This leads to findings of decreased visual acuity and, in turn, strabismus (ie, ocular misalignment) and/or nystagmus.
Question

E. Methacholine Challenge
This patient’s intermittent nocturnal dyspnea and episodic cough that began after a respiratory infection suggest a diagnosis of asthma, a disease characterized by airway inflammation and bronchial hyperreactivity to various stimuli, including physical, chemical, and allergenic irritants. Patients often have a family history of other diseases in the “allergic triad” (ie, allergic rhinitis, atopic dermatitis, asthma). Asthma is an obstructive airway disease (FEV1/FVC ≤70%); however, airflow obstruction is variable, and lung function studies may be normal between exacerbations.
Bronchoprovocation testing can be useful in diagnosis when a patient presents with a history concerning for asthma but has normal spirometry values. Methacholine is an inhaled muscarinic cholinergic agonist that induces bronchoconstriction; patients are given increasing doses followed by serial spirometry. Patients with asthma demonstrate hyperresponsivity to bronchoprovocation with a reduction in FEV1 at lower doses than in those without asthma.
Conversely, bronchodilator administration can help diagnose patients who have obstructive values on spirometry at baseline. Spirometry is performed before and after administration of a bronchodilator (eg, levalbuterol); reversal of the airflow obstruction after therapy suggests the diagnosis of asthma, while irreversible obstruction suggests an alternative diagnosis (eg, bronchiolitis, COPD). However, in a patient who is currently asymptomatic with normal lung function studies, this is unlikely to aid in diagnosis
Question

A. Control of Vector Arthropods
These patients have a febrile illness with signs of meningitis (eg, neck stiffness, headache) and encephalitis (eg, confusion, seizure, tremor, focal deficits), raising strong suspicion for an outbreak of arbovirus meningoencephalitis (eg, West Nile virus, La Crosse virus). Arboviruses are small RNA viruses that are harbored by birds and small mammals and are transmitted to humans via biting arthropods (eg, mosquitos, ticks, fleas), primarily during the summer months when arthropod populations are at their peak.
Infections in otherwise healthy individuals usually result in an asymptomatic low-level viremia that is cleared within a week by the humoral antibody response. In contrast, patients who cannot mount a rapid, effective antibody response (eg, elderly, immunocompromised) may have persistent and more severe viremia; these individuals often develop a severe flu-like illness (eg, fever, headache, fatigue, arthralgias) that may progress to meningitis and/or encephalitis.
Most arbovirus infections are self-limited and resolve with supportive care, but some cases of meningoencephalitis are fatal. Because no vaccines are currently available for North American arboviruses
Question

D. It is highly charged
A drug with a Vd of 4.5 L, which is approximately the same as the plasma volume, is likely to be highly bound to plasma proteins such as albumin. Binding to plasma proteins tends to retain drug in the plasma compartment and prevent the diffusion of drug into the extravascular compartments. If this drug were not bound to albumin, it would be more likely to diffuse into the interstitium and a higher Vd would be expected.
Question

A. CBC

Azathioprine is an immunosuppressant used in the prevention of organ transplant rejection and the treatment of autoimmune diseases, including rheumatoid arthritis, inflammatory bowel disease, and autoimmune hepatitis. It functions via inhibition of purine synthesis pathways. Following ingestion, azathioprine is converted to 6-mercaptopurine, which is then converted to 6-thioguanine metabolites; these metabolites are pharmacologically active and mediate both the therapeutic and adverse effects of azathioprine.
The 6-thioguanine metabolites reduce cellular proliferation via 2 methods of purine synthesis inhibition:
The metabolites inhibit phosphoribosylpyrophosphate (PRPP) amidotransferase, an enzyme that catalyzes an early step in de novo purine synthesis.
The metabolites act as false nucleotides, incorporating into actively replicating DNA and RNA and rendering the growing nucleic acid strand nonfunctional.
These effects are exerted preferentially on rapidly dividing cells (eg, activated lymphocytes in the setting of organ transplant or autoimmune disease) but are otherwise nonspecific and disrupt other hematologic cell lines, including neutrophils, erythrocytes, and platelets. Therefore, pancytopenia (ie, leukopenia, anemia, and thrombocytopenia) is a common adverse effect that must be monitored with periodic complete blood count testing.
A 24-year-old woman comes to the emergency department due to 2 days of fever. The patient has no chronic medical conditions, drinks alcohol occasionally, and does not use tobacco or illicit drugs. She is sexually active and frequently travels for her work as a freelance journalist. Temperature is 38.3 C (101 F), blood pressure is 118/66 mm Hg, pulse is 106/min, and respirations are 18/min. Physical examination is notable for mild scleral icterus and splenomegaly. Laboratory findings are shown in the exhibit. Which of the following infectious agents is most likely responsible for this patient’s current condition?

Plasmodium falciparum
This patient with fever, icterus, splenomegaly, and ring-shaped parasites within red blood cells has malaria, which is caused by 4 main species of Plasmodium (P falciparum, P vivax, P ovale, P knowlesi). Although malaria has been eradicated from the United States, cases still arise due to travel to endemic regions, particularly when no chemoprophylaxis is taken.
The parasite is transmitted by female Anopheles mosquitos during blood feeding, travels to the liver where it infects hepatocytes, and then subsequently undergoes asexual reproduction, which generates hepatic schizonts with thousands of daughter cells (merozoites). Rupture of the schizont into the circulatory system leads to erythrocyte infection and cycles of intraerythrocytic reproduction.
As the parasite disseminates throughout the circulation, production of inflammatory cytokines causes nonspecific symptoms (eg, fatigue, fever, malaise, headache) and, sometimes, life-threatening complications (eg, seizure, renal failure, circulatory collapse). Hepatosplenomegaly and signs of anemia and hyperbilirubinemia (eg, scleral icterus) are often present. The diagnosis is confirmed when peripheral blood microscopy shows intraerythrocytic trophozoites with a “diamond ring” appearance.
Question

E. Propranolol

Prolonged hypoglycemia can lead to irreversible neurologic deficits and death. To prevent injury, counterregulatory systems raise blood glucose in response to hypoglycemia via sympathetic nervous system activation (ie, norepinephrine/epinephrine release) and increase secretion of glucagon, cortisol, and growth hormone.
Symptoms of hypoglycemia fall into 2 general categories: neurogenic (autonomic) and neuroglycopenic.
Neurogenic symptoms are mediated via norepinephrine/epinephrine and acetylcholine release during sympathetic stimulation. Symptoms due to norepinephrine/epinephrine include tremulousness, tachycardia, and anxiety/arousal, whereas acetylcholine causes sweating, hunger, and paresthesias.
Neuroglycopenic symptoms are due to inadequate availability of glucose in the CNS and include behavioral changes, confusion, visual disturbances, stupor, and seizures.
This patient has reduced awareness of hypoglycemia, likely due to the use of a nonselective beta blocker (eg, propranolol) for chronic treatment of migraines and/or hypertension. Nonselective beta blockers attenuate the norepinephrine/epinephrine-mediated symptoms of hypoglycemia, but cholinergic symptoms (eg, hunger) are unaffected. In addition, nonselective beta blockers can contribute to the severity of hypoglycemia; epinephrine stimulates hepatic gluconeogenesis and peripheral glycogenolysis, but this effect is diminished by nonselective beta blockers.
Question

The patient’s contrast-enhanced CT scan shows multiple hypodense masses in the liver (arrows) consistent with metastatic liver disease. Metastases are the most common malignant neoplasms of the adult liver and are 20 times more common than hepatocellular carcinoma. The liver is the second most common site of metastatic spread (after the lymph nodes) because of its large size, dual blood supply, high perfusion rate, and the filtration function of Kupffer cells.
Patients with liver metastases typically have multiple nodules throughout the liver that may replace more than 80% of the hepatic parenchyma, often resulting in marked hepatomegaly. The nodules frequently outgrow their vascular supply and become centrally necrotic and umbilicated. Even with significant metastatic involvement, patients may have no clinical or laboratory signs suggestive of hepatic insufficiency. However, once the majority of the liver parenchyma is destroyed or the major bile ducts become obstructed with tumor, patients tend to present with jaundice or abnormal hepatic enzymes (eg, elevated aminotransferases, alkaline phosphatase).

Question

D. Increased ADH secretion

This patient likely has the syndrome of inappropriate antidiuretic hormone secretion (SIADH), the most common cause of hyponatremia following subarachnoid hemorrhage (SAH). Antidiuretic hormone (ADH) is normally released by the hypothalamus and posterior pituitary in response to elevated serum osmolality (eg, following water deprivation) or decreased arterial blood volume. ADH promotes renal water reabsorption, which leads to concentration of the urine, extracellular fluid volume expansion, and lowering of serum osmolality and serum sodium. Hypothalamic damage following SAH is thought to trigger excessive production of ADH, resulting in the classic SIADH features of hypotonicity (ie, low serum osmolarity), hyponatremia, and persistently concentrated urine (ie, high urine osmolality).
In addition to SIADH, hyponatremia after SAH can also be due to cerebral salt wasting (caused by increased secretion of brain natriuretic peptide, which leads to urinary sodium losses) or acute cortisol deficiency (eg, from pituitary injury, leading to hypotension) (Choice E). In both conditions, decreased extracellular fluid volume causes a secondary increase in ADH and worsening hyponatremia.
(Choice A) In primary polydipsia, defective central thirst regulation leads to excessive water intake and hyponatremia. ADH levels are low, rather than high. Primary polydipsia is typically seen with certain psychiatric conditions (eg, schizophrenia) or use of psychotropic medications. It is not commonly associated with SAH.
(Choice B) Impaired renal concentrating ability is seen in diabetes insipidus (DI), which occurs either due to ADH resistance (in nephrogenic DI) or decreased ADH production (in central DI). DI may follow cerebral injury; however, it does not cause hyponatremia. Rather, DI results in a clinical picture opposite that of SIADH, featuring hypernatremia, increased serum osmolality, and dilute urine (ie, low urine osmolality).
(Choice C) Inadequate dietary intake of sodium is a rare cause of hyponatremia primarily seen in cases of chronic alcohol abuse (eg, beer potomania). SIADH is a more likely cause of hyponatremia in this patient.
Question

D.

Ten days after surgery, this patient’s intact, healing surgical incisions are most likely undergoing a type of neovascularization called angiogenesis, the process by which new blood vessels sprout and grow into the wound from surrounding, uninjured vessels.
Angiogenesis primarily occurs during the proliferation phase of wound healing, which begins around day 3 (overlapping with the end of the inflammatory phase) and lasts approximately 5 weeks. During the proliferation phase, fibroblasts multiply and synthesize ground substance and type III collagen, which form an amorphous gel into which new capillaries can grow. In addition, fibroblasts secrete fibroblast growth factor and vascular endothelial growth factor, which stimulate endothelial cell proliferation, migration, and differentiation—leading to the formation of new capillaries.
By increasing the number of capillaries within the healing surgical incision, angiogenesis increases blood flow to the area, causing the pink and slightly warm characteristics of the wound at this stage. The incision’s newly formed epithelium (ie, reepithelialization) typically has a shiny appearance as well.
Phases of wound healing

Hemostasis phase of wound healing timing and features
0 - hours - 1 day
Platelets
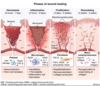
Inflammation phase of wound healing timing and features
3 hours - 5 days
Macrophages

Proliferation phase of wound healing
3 days - 5 days
Fibroblasts
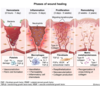
Remodeling phase of wound healing timing and features
3 weeks - 2 years
Matrix metalloproteinases

Question

F. White blood cell casts

This patient has urinary frequency and urgency consistent with a urinary tract infection (UTI). Women are more susceptible to UTIs because the female urethra is closer to the rectum and shorter than the male urethra. Sexual intercourse is often a precipitating factor because it introduces enteric bacteria to the periurethral area, leading to ascending infection of the bladder.
UTIs are categorized into either upper (eg, pyelonephritis) or lower (eg, cystitis) infections based on the ascension of bacteria through the urinary tract. Pyelonephritis and cystitis can share concomitant clinical features including dysuria, suprapubic pressure, and hematuria. Urinalysis with microscopy is often performed to confirm the diagnosis of UTI, but both upper and lower UTIs can show hematuria, pyuria (presence of urine white blood cells [WBCs]), and bacteriuria (Choices A and D).
However, the presence of WBC casts on urinalysis differentiates between upper and lower UTIs and can confirm the diagnosis of pyelonephritis. This is because WBC casts are formed only in renal tubules, where WBCs precipitate with Tamm-Horsfall protein secreted by tubular epithelial cells. WBC casts can also be seen with other intrarenal disorders (eg, acute interstitial nephritis), but urinary frequency and urgency are not typically present.
How to differentiate between upper and lower UTI
However, the presence of WBC casts on urinalysis differentiates between upper and lower UTIs and can confirm the diagnosis of pyelonephritis. This is because WBC casts are formed only in renal tubules, where WBCs precipitate with Tamm-Horsfall protein secreted by tubular epithelial cells. WBC casts can also be seen with other intrarenal disorders (eg, acute interstitial nephritis), but urinary frequency and urgency are not typically present.

Question

A.

Aminoglycosides (eg, gentamicin, tobramycin) are bactericidal antibiotics that bind to the 30S ribosomal subunit and inhibit protein synthesis. They are commonly used for severe gram-negative infections but carry a significant risk of acute kidney injury. Aminoglycosides are filtered across the glomerulus and concentrate within the proximal renal tubules, where they impair lysosomal function, protein synthesis, and mitochondrial activity, leading to acute tubular necrosis (ATN). This is visualized histologically as focal tubular epithelial necrosis, often with extensive granular casts that obstruct the tubular lumen and lead to rupture of the basement membrane.
Aminoglycoside-induced kidney injury typically manifests within 1 week of therapy initiation. Due to the high intratubular drug concentrations, ATN can occur despite normal serum drug levels. Proximal tubular dysfunction results in loss of resorptive capacity and electrolyte wasting (eg, hypomagnesemia, hypophosphatemia); severe disease can result in Fanconi syndrome (ie, aminoaciduria, glucosuria, uricosuria, phosphaturia). Distal tubular injury may also occur and results in loss of concentrating capacity with polyuria (nonoliguric renal failure). Urinalysis typically demonstrates mild proteinuria with granular or hyaline casts. Consistent with other causes of ATN, the fractional excretion of sodium (FENa) is >2%.
Sites of acute tubular necrosis
