urogentital Flashcards
Schematic summary of endocrine events, behavioral and vulvar changes, and changes in the vaginal smear during the estrus cycle in bitches

A working cannula is inserted on the midline 30 mm caudal to the umbilicus in a medium- to large-breed dog, to introduce the laparoscope. Two additional midline cannulas are placed under direct (laparoscopic) visualization at 30 to 50 mm cranial to the umbilicus and 30 to 50 mm cranial to the pubis in large-breed dogs (Figure 109-5). If a prophylactic gastropexy is performed in conjunction with ovariohysterectomy, the cranial portal may be placed 30 to 50 mm to the right of midline and 30 to 50 mm caudal to the last rib and subsequently used for the gastropexy after completion of the ovariohysterectomy




Developmental anomalies of the vestibulovaginal junction include focal hypoplasia (A), imperforate hymen (B), vertical septum (C), and double vagina (D).

Vulvovaginectomy may be performed to achieve complete resection of vaginal neoplasia. A, The proposed incision around the vulvar margin is outlined in blue. B, The vascular supply to the vagina is ligated during resection, and the urethral blood supply is preserved. C, Resection of the genital tract is completed through a caudal approach. A stay suture is placed on the urethra before transection. The urethral mucosa is then sutured to the skin to create a permanent perineal urethrostomy. Remaining tissues are closed routinely.




Schematic drawing of the descent of the testis in the dog. (1) Testis; (2) epididymis; (3) gubernaculum; (4) cremaster muscle; (5) peritoneum; (6) internal abdominal oblique; (7) external abdominal oblique; (8) inguinal canal; and (9) vaginal cavity.


root of the penis with superficial muscles, right lateral aspect




Normal urethral meatus and types of hypospadias: glandular, penile, scrotal, perineal, and ana

Partial penile amputation. A, The penis is extruded from the prepuce and catheterized. The prepuce is retracted with umbilical tape, and a tourniquet is placed around the penis. The penis is incised to create two flaps. B, The urethra is transected distal to the proposed ostectomy site after it has been dissected from the groove of the os penis. The os penis is trimmed with a rongeur. C, Cavernous tissue on the dorsal aspect of the penis is closed with fine absorbable sutures placed in the tunica albuginea. The urethral margin is sutured to penile epithelium with simple interrupted absorbable sutures.

Technique for shortening of the prepuce in conjunction with partial penile amputation. A, A rectangular portion of prepuce is excised. B, A sliding skin flap facilitates retraction of the cranial prepuce (arrows). C, The segments are apposed with two layers of suture.

Ablation of the external male genitalia. A, The skin is incised around the sides or base of the prepuce and scrotum. B, The penis is separated from the body wall, and its blood supply is temporarily occluded with a ligature or tourniquet proximal to the proposed transection site. The penile body is sharply severed. C, After hemostasis has been achieved, the tunica albuginea is apposed over the end of the transected penis. D-E, A urethrostomy is performed, and the remaining skin defect is closed

Phallopexy for treatment of paraphimosis. A, A full-thickness skin incision is made into the preputial cavity. B, A strip of mucosa (0.5 × 1.5 cm) is excised from the dorsal midline of the prepuce and dorsal aspect of the penis 2 cm caudal to the penile tip. C, The defects of the penis and prepuce are apposed to each other with simple interrupted sutures of 3-0 or 4-0 absorbable monofilament. The preputiotomy is then closed in two or three layers

Preputial advancement. A, A crescent-shaped section of skin is removed cranial to the prepuce. B, Preputial muscles can be resected and reapposed or plicated and secured with suture. C, The subcutaneous tissues and skin are closed routinely



Renal biopsy. A, Monopty biopsy needle with biopsy guide attached. B, To obtain a biopsy of the kidney, the biopsy instrument is advanced until it penetrates the capsule. The biopsy needle is positioned to take a biopsy of the renal cortex. The needle should be aimed so that it travels across the cortex (left) and not into the medulla (right) where it could damage vessels

Kidney anatomy
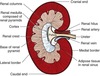
Semischematic drawing of the canine kidney (A). The papillae have joined in an irregular common crest; the thickenings of the crest alternate with recesses of the renal pelvis as shown by the corrosion cast of the pelvis

Nephrotomy. A, After vascular occlusion, the kidney is incised longitudinal through the capsule on midline of the convex surface. The cortex is cut for a bisectional nephrotomy or spread (B) for an intersegmental nephrotomy. C, The exposed calculus is grasped and removed. The pelvic recesses are explored and flushed, and a catheter (D) or suture is passed through the ureter to verify patency. E, The nephrotomy incision is closed by placing sutures through the renal capsule and superficial parenchyma

Partial nephrectomy. A, If possible, the capsule is peeled back from the area to be resected. B, Overlapping mattress sutures are passed through the parenchyma proximal to the proposed line of resection. C-D, The sutures are tightened to approximate the tissue, and the parenchyma is excised distal to the sutures. If possible, the capsule is reapposed over the resected parenchyma.






Pelvic cavity of the female dog. 1, Caudal mesenteric plexus; 2, right and left hypogastric nerves; 3, caudal mesenteric artery; 4, caudal mesenteric ganglion; 5, aorta; 6, psoas minor; 7, lateral cutaneous femoral nerve; 8, abdominal oblique muscles; 9, deep circumflex iliac artery; 10, external iliac artery; 11, internal iliac artery; 12, quadratus lumborum (cross-section); 13, iliopsoas; 14, femoral nerve; 15, sacroiliac articulation; 16, caudal gluteal artery; 17, lumbar nerves 6 and 7; 18, first sacral nerve; 19, second sacral nerve; 20, third sacral nerve; 21, pelvic nerve; 22, caudal cutaneous femoral nerve; 23, pudendal nerve; 24, coccygeus; 25, levator ani; 26, perineal nerve and artery; 27, pelvic plexus; 28, artery and nerve to clitoris; 29, urethra; 30, vagina; 31, urethral branch of vaginal artery; 32, caudal vesical artery; 33, bladder; 34, vaginal artery; 35, cranial vesical artery (variable presence); 36, internal pudendal artery; 37, ureter and ureteral branch of vaginal artery; 38, umbilical artery; 39, uterine artery; 40, uterine horn; 41, descending colon.

Prescrotal urethrotomy. The retractor penis muscle is retracted laterally, and the urethra is incised on midline just caudal to the os penis

erineal urethrostomy in the male dog. A, The dog is placed in a perineal position with the tail pulled forward. B, The retractor penis muscle is exposed and retracted, and the urethra is incised on the midline. C, A catheter is advanced to the level of the obstruction. D, For urethrotomy, the urethra is closed with 4-0 or 5-0 monofilament absorbable suture in a continuous pattern. E, For urethrostomy, the urethral mucosa is sutured to the skin in a continuous or interrupted pattern

Scrotal urethrostomy in a male dog. A, An elliptical incision is made at the base of the scrotum, retaining enough skin to allow for a tension-free closure of the urethrostomy. B, Castration is performed routinely if the animal is intact. C, A urinary catheter is placed retrograde from the penile orifice to help identify the urethra. The retractor penis muscle is dissected off the urethra and retracted laterally. D, A sharp incision is made on the ventral midline of the urethra using a scalpel blade; the incision is enlarged with iris scissors approximately 2.5 to 4 cm (inset). E, The urethral mucosa is sutured to the skin using a simple interrupted or continuous pattern. Suture includes the entire thickness of urethra and split-thickness skin

Perineal urethrostomy in a male cat. A, The patient is placed in sternal recumbency with a purse-string suture in the anus. An incision is made encircling the scrotum and prepuce. Castration is performed routinely if the animal is intact. The penis is retracted from the incision to allow dissection of the subcutaneous tissues to the level of the pelvis. B, The penis is freed of its attachments to the pelvis. The origin of the ischiocavernosus muscle is identified, severed, and elevated from the ischium. C, The ligament of the penis found ventral to the penis is severed. D, Dissection is continued laterally and dorsally to expose the retractor penis muscle, bulbourethral glands, and bulbocavernosus muscle. E, The retractor penis muscle, or its remnant in castrated males, is removed from the dorsal aspect of the penile urethra. F, The urethra is incised on the dorsal midline beginning distally and continuing to the level of the bulbourethral glands. G, The urethral mucosa is sutured to the skin beginning at the most dorsal aspect of the urethral incision. The dorsalmost sutures (at the 10, 12, and 2 o’clock positions) are preplaced in an interrupted pattern to adequately spatulate the opening. H, The urethra is sutured for a distance of 1 to 1.5 cm, in a simple interrupted or continuous pattern alternating sides. If necessary, the skin dorsal to the urethrostomy site is closed separately. I, A mattress suture is placed around the cavernous tissue to control hemorrhage. J, The remaining distal penis is amputated. K, Sutures are placed through the corners of the termination of the urethrostomy, and the remaining skin wound ventral to the urethrostomy is closed routinely. L, Completed perineal urethrostomy. A figure of eight suture pattern (inset) is used for urethrostomy closure to position knots away from the incision but maintain accurate urethra–skin apposition

Prepubic urethrostomy in a female dog (A, inset). The dashed line shows the proposed incision site for ventral celiotomy. A, Exposure of urethra and bladder shows the proposed site of urethral transection. B, The distalmost part of healthy intrapelvic urethra is transected. C, The urethra is drawn through the abdominal incision or a separate stab incision 2 to 3 cm paramedian (shown) (inset). The urethra is spatulated, and the urethral mucosa is sutured to the skin with interrupted suture

Penile hypospadias in a dog.

Urethral prolapse in a young male dog

Urethropexy for urethral prolapse. A, A groove director is inserted in the urethra to guide suture placement. Suture is passed through the penile body and out the urethra and then back through the urethra and out the penile body. B, Tightening the suture inverts the urethral mucosa
