Week 5: Toxin-mediated infections Flashcards
What is a bacterial toxin?
PRotein or lipopolysaccharide toxin secreted by or remaining a component of the bacteria
What is an exotoxin?
Toxin secreted by bacteria
What is an endotoxin?
Toxin that remains a component of bacteria (eg in the cell membrane)
Examples of exotoxins
- Diptheria toxin
- Pertussis toxin
- Shiga toxin
- Botulinum toxin
- Tetanus toxin
Examples of endotoxins
- LPS in gram negative bacteria
- Normally lipopolysaccharide complexes
Tropism of toxins
eg
- neurotoxin indicates nervous system
- enterotoxin indicates GI tract
Protein toxin components
- protein toxins often have 2 components (A and B units)
- one bind to a receptor and another with enzymatic capabilities
Examples of toxins involved in invasive infections
- Spe B in necrotizing fasciitis
Toxins that commonly cause problems from a distance WITHOUT invasion
- Botulism
- Tetanus
Question
What is the most potent toxin?
A. Strychine
B. Rattlesnake Venom
C. Botulinum toxin
D. Tetanus toxin

C. Botulinum toxin
Relative toxin potencies

Clinical case

Necrotizing Fascitis (often associated following varicella)

Toxin mediated disease NOT associated with a single organism
Necrotizing fasciitis
How does necrotizing fasciitis present?
- Rapid spread (hours)
- Initially pain is out of proportion
- Appear sicker than one might expect
- As disease progresses pain lessens (nerves destroyed)
- Progressively worse local perfusion (capillaries destroyed)
- ‘Brawny’ edema of the affected site (feels like wrestling mat on skin)
- Frequent sepsis/hypotension
Toxins with a potential role in Necrotizing Fasciitis
- Leukocidin
- Exfoliatin B
- Streptolysin O
- Streptococcal pyrogenic exotoxin E
- Streptococcal pyrogenic exotocin B
Organisms that produce toxins in necrotizing fasciitis
- S. aureus
- S. pyogenes
Toxins produced by S. aureus in necrotizing fasciitis
- Leukocidin
- Exfoliatin B
Toxins produced by S. pyogenes in necrotizing fasciitis
- Streptolysin O
- Streptococcal pyrogenic exotoxin E
- Streptococcal pyrogenic exotoxin B
Leukocydin is produced by?
S. aureus
Exfoliatin B is produced by?
S. aureus
Streptolysin O is produced by?
S. pyogenes
Streptococcal pyrogenic exotoxin E is produced by?
S. pyogenes
Streptococcal pyrogenic exotoxin B is produced by?
S. pyogenes
Leukocidin toxic effect
Destruction of phagocyte membranes
Exfoliatin B toxic effect
epidermal cleavage
Streptolysin O toxic effect
Destruction of cholesterol
Streptococcal pyrogenic exotoxin E toxic effect
Superantigen formation
Streptococcal pyrogenic exotoxin B toxic effect
Cysteine protease
Mortality rate of necrotizing fasciitis in adults
24%
Mortality rate of necrotizing fasciitis in pediatric
10%
Mortality rate of necrotizing fasciitis in neonates
50%
Necrotizing fasciitis how many organisms in adults?
most are polymicrobial infections
Necrotizing fasciitis how many organisms in pediatrics?
Most are monomicrobial Group A Strep
Necrotizing fasciitis is commonly associated with the development of?
Toxic Shock Syndrome
Treatment of Necrotizing Fasciitis
- QUICK to surgery for debriding
- Also antibiotics

Question


Why does Necrotizing Fasciitis present the way it does?

The most important thing in treating Necortizing Fasciitis
Time to surgery (GET THERE QUICK)
Empiric Antibiotics to treat Necrotizing Fasciitis

Clinical case

Toxic Shock syndrome

What is this depicting?

palm & sole involvement
What is toxic shock syndrome?
- caused by S. aureus or S. pyogenes
- S. aureus secretes TSST (Toxic Shock Syndrome Toxin)
- S. pyogenes secretes pyrogenic exotoxins
- TSST binds to both MHC II complex and T-cell receptors
- This binding activates the T-cells 2000 fold more than traditional binding in the cleft leading to a cytokine storm with resultant shock, capillary leak, multi-organ system failure, etc.
Describe TSST toxic effect
- Toxins bind to both MHC II complex and T-cell receptors
- This binding activates the T-cells 2000 fold more than traditional binding in the cleft leading to a cytokine storm with resultant shock, capillary leak, multi-organ system failure, etc.

Treatment of Streptococcal Toxic-Shock Syndrome
- Debride
- Antibiotics (IV until afebrile transition to oral)
- Peniciilin for Strep
- Clindamycin to reduce toxin production
- IVIG may be considered (to bind up toxin)

Staphylococcal Toxic-Shock Syndrome Diagnostic Criteria Acronym
- Skin (rash, desquamation)
- Temperature elevation
- Absence of alternative dx (eg RMSF, lepto, measles)
- Poly-system involvement (>=3)
- Hypotension

Staphylococcal Toxic-Shock Syndrome Treatment
- IVIG (bind toxin)
- Antibiotic for staph
- Clindamycin to reduce toxic production
- Supportive care

Question

D. only about 20% of Staph carry the gene for TSST
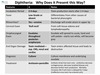
Question


How does Diptheria present
- Low grade or afebrile
- Erosive rhinorrhea (discharge will erode ulcers in upper lip)
- ‘Bull neck’ from soft tissue edema and lymphadenopathy
- Exudates throughout the poterior oropharynx will spread to uvula, hard and soft palate–starts out whitem will become grey)
- End-organ damage (toxin-mediated, toxin enters affected tissue and leads to destruction)
Story about Bordatell Pertussis
Benjamin Franklin didn’t vaccinate

Pertussis deaths by age

Question

E.

Clinical Case


Presentation of Tetanus
Tetanospasmin is a neurotoxin produced by all toxigenic strains
Released at the site of infection where it spreads throughout the body
It affects the nerve endings of inhibitory neurons in the central nervous system
- Inhibits release of inhibitory neurotransmitters (ie GABA and glycine) resulting spasm
- Functional denervation of lower motor neurons
- Muscles with the shortest neural pathways are affected first
- Lockjaw
- Risus sardonicus (Sarcastic smile)

Opisthtotonus AKA

Botulism vs Tetanus

Question

D. $45K

Efficacy of Baby BiG

Anthrax caused by?
Bacillus anthracis

Question


ARS question

Clinical distribution of human anthrax cases

Anthracis toxins mechanisms
- Two exotoxins
- Lethal toxin
- Edema toxin
- Internalized by cells
- Lethal toxin inhibits protein-kinase mediated signal transduction in the cell
- Edema toxin increases cAMP levels causing dysregulation of cellular physiology and edema
