Neurology Flashcards
(13 cards)
DDx for working diagnosis of CVA/TIA - 7
Gestalt CLIMBS during possible stroke!
- Glucose low (hypOglycemia)
- Conversion disorder
- Lesion in brain (tumor, AVM, aneurysm, hemorrhage)
- Infection (abscess, septic emboli)
- Migraine complicated
- Bell’s palsy
- Seizure (postictal paralysis)
these are dx that mimic stroke
What’s the most important component of history for working diagnosis stroke?
ONSET of sx AS ACCURATE AS POSSIBLE
You suspect a pt had a Stroke
After FIRST, ruling out Hemorrhagic stroke with _____, when should thrombolytic therapy be given? What should be given?
NonContrast Head CT; WITHIN 3 HOURS OF SX ONSET! ; IV Alteplase

tPA DeConverts plasminogen –> plasmin –> catabolizes Fibrin into Fibrin split products
What is the interpretation for the NIH stroke scale?
> 4 is where tPA candidates generally fall

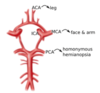
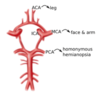
CP for an Anterior cerebral artery infract
uL LE > UE weakness/numbness contralaterally

CP for an Middle cerebral artery infract - 2
- uL Face and UE > LE weakness/numbness contralaterally
- +/- [aphasia if dominant hemisphere] or [neglect if non-dominant]
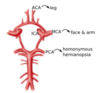
CP for an Posterior cerebral artery infract
Homonymous Hemianopsia
CP for an Vertebralbasilar artery infract - 7
The 7 D’s
- DEC level of consciousness
- Diplopia
- Droopy face
- Dysarthria
- Dysphagia
- Dysmetria
- Dysequilibrium
Describe the Lacunar Syndrome CP
lenticulostriate vessels perfuse [Be TIPC] (not Pons)
Lacunar Stroke= [Thrombotic HTN Arteriolosclerosis & Thrombotic microatheromas] of lenticulostriate vessels –> [cystic infarcts < 15 mm] –> Lacunar Syndrome
1A: Basal Ganglia–>Hemiballismus & involuntary writhing
1B: [Internal Capsule-POST limb/Pons/Corona Radiata]–> pure Motor stroke vs ataxia vs. clumsy hand-dysarthria
1C: ThalamuS VPL –> CTL Sensory Stroke
VPL=VentroPosteroLateral nc

You suspect a pt had a Stroke
What’s the maximum time it should from the time the Pt enters the ED Door until…
Seeing You (physician)
Seeing the Stroke Team
Labs are completed
NonContrast Head CT is completed
Admission to hospital
Stroke Labs = CBC, CMP, PTT/PT, EKG, CXR, UA
Remember: Your Gestalt CLIMBS during possible stroke

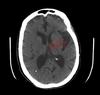
When’s the soonest you’d see any possible findings of acute ischemic stroke radiographically? - 2 ; What would you see?
3 hours; HYPERdensity representing acute thrombous/embolus in major vessels (MCA and vertebrobasilar) +/- loss of cortical gray/white differentiation

remember, your Gestalt CLIMBS during possible stroke
You suspect a pt had an ischemic Stroke and because they’ve arrived to the ED within ___ hours, you’ve given IV Alteplase tPA
Now that they’re on tPA, what is their BP goal? ; What is the BP goal for stroke pts who don’t receive IV Alteplase
3 hours ; < 180/105 for first 24 hours after getting tPA ; < 220/120

Remember: Your Gestalt CLIMBS during possible stroke
Recommenations for Aspirin usage in acute ischemic stroke pts - 2
- Give ASA within 48 hrs of stroke sx if they DONT get tPA
- Give ASA 24 hours after tPA if they end up getting tPA
