What are some S/S of a prodrome of syncope? (pt. position, pt. feelings, pt. appearance, pt. actions, pt. experience).
Pt. usually upright at beginning of attack (standing/sitting).
Pt. feels queasy, giddy, apprehensive, may sway, may get H/A.
Pt. appears pallor, ashen-gray color in face.
Pt. face/body perspiration, salivation, epigastric distress, nausea, vomiting.
Pt. may suppress symptoms by yawning, sighing, breathing deeply.
Pt. vision may dim or close, ears may ring, “grayout”-impossible to think clearly.
What is syncope (what occurs, how is recovery classified)?
Syncope: LOC and loss of postural tone, usually leading to recumbent position.
Recovery is rapid w/o confusion, H/A, or focal neuro symptoms, fatigue is common.
Convulsive syncope can result if recumbency is prevented.
How is blood to brain controlled, generally?
Brain autoregulates to maintain flow.
Heart under sympathetic/parasympathetic control.
Peripheral vasculature under sympathetic control.
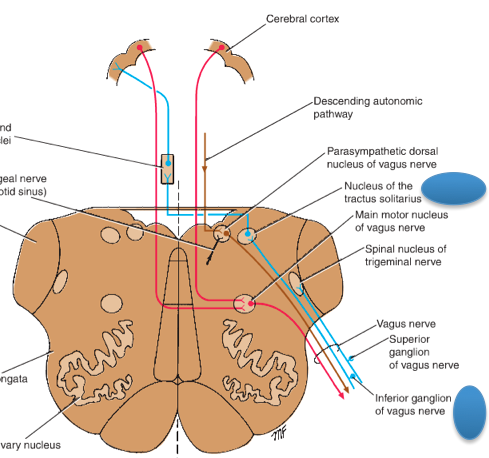
What role does the Nucleus Tractus Solitarius have on control of blood flow to the brain?
Response to increased baroreceptor activity:
- decreased HR (PNS, vagus).
- Relax peripheral vasculature by stopping sypathetic activity.
What are the 3 main categories of causes of syncope? Which is most common?
1) Neurogenic vasodepressor
2) Failure of sympathetic innervation of blood vessels and of autonomically activated compensatory responses
3) Diminished cardiac output
Most common - not categorized
Vasovagal - next most common
Describe what happens in neurogenic vasodepressor (what starts this process, what does it result in, where is the integrating center for all this control of blood flow)?
Stimulus sends signal to brainstem, triggers reflexive cessation of sympathetic activity.
Same time - increase in vagals activity -> bradycardia. (perspiration, increased peristaltic motility, nausea, and salivation).
All signals go into and out of nucleus tractus solitarius.
A category of neurogenic vasodepressor syncope is vasodepressor sycope. How is this classified, examples of triggers, what occurs with blood flow and how, what usually occurs in the heart?
The common faint.
Trigger could be pain from viscera, injury, etc.
Vessels controlled by sympathetic nervous system dilate -> blood goes to periphery instead of brain -> heart does not compensate by increaseing output.
Bradycardia is generated but is not essential for this type of syncope.
Another category of neurogenic vasodepressor syncope is neurocardiogenic syncope. Describe this type of syncope (what is it caused by).
Rapid contractions of left ventricle with deficient filling of the heart.
Signals from left ventricle lead to bradycardia and vasodilation.
Another form of syncope under the neurogenic vasodepressor category is glossopharyngeal neuralgia related syncope. How is this type of syncope caused? (how is it induced, what is the reaction, what is the result).
Pain localized in base of tongue, pharynx, larynx, tonsillar area.
Pain stimulates 9th cranial nerve leading to activation of medullary vasomotor centers via collaterals from NTS.
Pain -> bradycardia -> syncope.
Lastly, we have another type of neurogenic vasodepressor syncope called carotid sinus hypersensitivity. What causes this type of syncope?
Tight collar, neck pressure -> triggers bradycardia, hypotension or both.
Oversensitive, high pressure mechanoreceptors in the carotid sinus (particularly in stiffened, atherosclerotic blood vessels).
When talking about failure of sympathetic innervation of blood vessels and of autonomically activated compensatory responses causing syncope, what are some examples of how this?
Orthostatic hypotension: failure of ANS to increase peripheral resistance (TPR) or cardiac output.
Peripheral neuropathy: impair vasoconstriction or postural reflexes.
Pure autonomic failure (PAF): slow progressive degeneration exclusive to ANS, Lewy body inclusions in autonomic and enteric ganglia, disabling OH.
What are micturition syncope, and tussive + valsalva syncope?
Micturition syncope: vasoconstriction w/ full bladder then vasodilation when urinating, combined with postural hypotension, alcohol/ hunger/ fatigue/ valsalva can contribute.
Tussive + valsalva syncope: increased intrathoraci pressure -> block venous return. Ex: cough (tussive) + laughter associated.
Comparing LOC with syncope vs. seizure, name the differences regarding timing, prodrome, urinary incontinence, return to consciousness, mental confusion/ ha/ drowsiness, EEG.
Timing: seizure can occur anytime, syncope not usually while in recumbent position.
Prodrome: seizures have little forewarning (auras are brief), pallor usually precedes syncope.
Urinary incontinence: occurs often w/ seizure, occasional w/ syncope.
Return of consciousness: slow after seizure, fast after syncope.
Mental confusion etc.: symptoms found after seizure, not syncope.
EEG: abnormal between seizures in most cases, normal with syncope.
Regarding Gastaut + Fischer-Williams study on EEG changes in syncope, briefly describe the findings.
3-6sec cardiac pulses have no EEG change -> 7-13sec of cardiac arrest: LOC, pallor, muscle relaxation -> end of this period there are theta/ delta EEG waves in frontal lobes -> beyond 14-15sec EEG was flat for 10-20sec, large amplitude delta waves w/ tonic spasms -> 20-30sec after EEG reverted to normal.
