Core Lecture Series Flashcards
1
Q
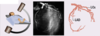
Describe the image

A
RAO Caudal
- LAD (on top)
- CFx (coming towards front)

2
Q
Describe the image

A
LAO Cranial

3
Q
Describe the findings
A

4
Q
Describe the findings

A
LAO Straight

5
Q
Describe the findings

A
LAO Cranial

6
Q
Describe the findings

A
RAO Straight

7
Q
What are the branches of the SMA?
A
- inferior pancreaticoduodenal
- intestinal
- ileocolic
- right colic
- middle colic
8
Q
What are the branches of the celiac trunk?
A
- Left gastric
- Common hepatic
- Splenic
9
Q
Describe the views and imaging of the left coronary system
A

10
Q
Describe the image

A

11
Q
Describe the image

A

12
Q
Describe the image

A

13
Q
Describe the image

A

14
Q
Describe the image

A

15
Q
Describe the image

A

16
Q
Describe the image

A

17
Q
Describe the views and imaging of the right coronary system
A

18
Q
Describe the image

A

19
Q
Describe the image

A

20
Q
Describe the image

A

21
Q
Describe the findings of the LV gram

A
