Vascular Disease Flashcards
Describe the findings

DVT
- US images:
- thin walled vein + not collapsible with compression –> DVT

What are other significant doppler/US findings of LE DVT?
- anechoic thrombus
- increased venous diameter
- loss of phasic flow with breathing
- augmentation with calf squeeze
- absence of color flow
Describe US findings:
- Baker’s cyst
well-circumscribed mass + echolucent center
Describe US findings:
- arterial stenosis
- atheroma and stenosis are visualized
- confirmed by spectral Doppler –>
- significant increase in velocities (flow accelearation)
Describe US findings:
- Polyarteritis nodosa
- small aneurysms
- beads of a rosary (“rosary sign”)
- most commonly involved organ = kidney
How does large artery atherosclerosis lead to cerebral ischemia?
- thromboembolism from the atherosclerotic plaque
-
direct occlusion of the penetrating arteries by the plaque
- especially in the case of intracranial atherosclerosis
- hemodynamic perturbations <– plaque related stenosis
What is the Class I indication for carotid endarterectomy?
TIA / CVA « 6 months secondary to –>
moderate to severe ( ► 50% stenosis ) extracranial carotid stenosis
What is an alternative to carotid endarterectomy?
- symptomatic ( CVA / TIA « 6 months)
- moderate-severe ( ► 50% stenosis)
Endovascular stenting (Class IIa)
- should be reserved for highly selected cases with:
- extracranial vertebral artery stenosis
- limited evidence
Describe the difference in treatment and outcomes for intracranial atherosclerotic disease:
- medical therapy
- endovascular stenting
- stenting has worse outcomes compared to best medical therapy
- should only be performed when best medical therapy has failed
What are the recommended first line antiplatelet therapies for secondary prevention of ischemic stroke?
- ASA
- Clopidogrel
- ASA/extended-release dipyridamole
****DAPT is not recommended over monotherapy with any of these agents
What is the mortality rate associated with?
- Type A aortic dissection
- aortic root / SoV involvement
- Without operation:
- First 24 hours –> 1-2% / hour
- First 48 hours –> 50%
What is the mortality associated rate?
- Type B aortic dissection
- In-hospital –> 8%
- 5 years –> 60-80%
Describe the initial treatment strategy for acute aortic dissection?
- Decrease wall stress by controlling:
- HR
- LV contractility
- change in pressure / change in time [dP / dT]
- Beta blockers
What BB’s are utilized in the acute aortic dissection?
- Metoprolol
- Labetalol
- Esmolol
- Propanolol

What are the indications for TEVAR in type B aortic dissection?
- Malperfusion syndrome (end-organ ischemia)
- Early expansion
- Rupture
- Refractory pain
What are the indications for surgery?
- Acute
- Type A dissection
All patients
What are the indications for surgery?
- Acute
- Type B dissection
- Rupture
- Rapid Aneurysm Expansion
- Extension
- Malperfusion syndrome
- Marfan Syndrome?

What are the indications for surgery?
- Chronic
- Type A dissection
- ► 5.5 cm
- ► 1 cm / year increase in dimension
- Severe AR
- Symptoms suggestive of:
- expansion or
- compression

What are the indications for surgery?
- Chronic
- Type B dissection
- ► 6 cm
- ► 1 cm / year increase in dimension
- Symtpoms suggestive of:
- expansion or
- compression

What are three genetic risk factors / mutations for aortic aneurysm and dissection?
- FBN1
- fibrillin-1 gene
- Marfan’s syndrome
- TGFB1-2
- transforming growth factor beta 1 and 2 gene
- Loeys-Dietz syndrome
- COL3A1
- Collagen type 3 alpha 1 gene
- Vascular Ehlers-Danlos
What patients are at increased risk of PAD?
- Age ► 65 years
- Age 50-65 years + risk factors (DM, tobacco abuse, dyslipidemia, HTN) or FH PAD
- Age < 50 years + DM and 1 additional risk factor for atherosclerosis
- Known ASCVD in another bed
- coronary, carotid, subclavian, renal, mesenteric artery stenosis, AAA
Describe the diagnostic testing algorithm for suspected PAD?

What is the next step?
- history or PE suggestive of PAD
- ABI > 1.4 (noncompressible vessels)
Toe-brachial index (TBI)
- « 0.70 = abnormal
What is the mortality associated with a diagnosis of PAD?
- 5- year risk of CV death –> 25-30%
- Nonfatal MAACE –> 20%
What are the benefits of exercise ABI?
- Diagnosing PAD in patients with:
- claudication and
- normal ABI at rest
- Discriminating claudication from pseudoclaudication
- Assessing functional capacity
What constitutes further anatomic assessment in PAD?
When should this be performed?
- Duplex US, CTA, MRA or invasive angiography
- Performed with revasculrization is planned
What patient should be screened for PAD?
- 52-year old woman with pale feet when lying in bed, reddish color when standing
- 84-year-old woma with a draining ulcer over the medial malleolus
- 73-year-old man with pain and tingling in both legs while walking, reduced with bending forward
1. - 52-year-old woman with pale feet when lying in bed, reddish color when standing
- elevation pallor and dependent rubor –> PAD
- 84 year old with draining ulcer –> venous insufficiency ulcers
- arterial ulcers tend to be dry
- 73-year old with tingling in both legs bending over
- neurogenic claudication –> spinal stenosis
Describe the findings

Raynaud phenomenon
- exaggerated vascular response to cold temperature or emotional stress
- Secondary RP - triggers:
- Autoimmune diseases
- systemic sclerosis
- SLE
- mixed connective tissue disease
- Sjogren syndrome
- dermatomyositis/polymyositis
- Drugs / Toxins
- BB
- Clonidine
- Sympathomimetics
- Stimulants (Methamphetamines)
- Cyclosporine
- Cisplatin
- Bleomycin
- Autoimmune diseases

What are the indications for carotid duplex prior to CABG?
- > 65 years of age
- LM stenosis
- PAD
- Tobacco abuse (history of)
- TIA/CVA (history of)
- Carotid Bruit
Describe the findings

Cholesterol emboli syndrome (CES)
- nonspecific symptoms
- livedo reticularis
- renal failure
- mesenteric ischemia
- Treatment:
- supportive
- increase statin therapy

What is the most common cause of atheroembolism?
iatrogenic - > 70%
- secondary to catheter-based angiography or vascular surgery
What is diagnostic of obstructive PAD on exercise ABI?
decrement of > 20%
- functional testing is important to evaluate for PAD in patients with exertional symptoms (Class I)
Describe diagnostic testing, findings and treatment of ALI:
- Category I: Viable limb
- Dopplers:
- Audible arterial
- Audible venous
- Category I: Viable limb
- Normal motor function
- No sensory loss
- Intact capillary refill
- Urgent (Class I)
- Anticoagulation
- Revascularization

Describe the diagnostic/treatment algorithm for ALI

Describe diagnostic testing, findings and treatment of ALI:
- Category IIa: Marginally threatened
- Dopplers:
- Inaudibale arterial
- Audible venous
- Motor/Sensory function assessment:
- Intact motor function
- Sensory loss limited to toes if present
- slow-to-intact capillary refill
- Emergent (Class I) - salvageable if treated promptly
- Anticoagulation
- Revascularization

Describe diagnostic testing, findings and treatment of ALI:
- Category III: Irreversible
- Dopplers:
- Inaudibale arterial
- Inaudible venous
- Motor/Sensory function assessment:
- Complete loss of motor function
- Complete sensory loss
- Absent capillary refill
- Emergent (Class I)
- Primary amputation

Describe the findings post-PCI?
What is the best way to confirm the diagnosis?

- Cholesterol Embolization Syndrome (CES)
- Biopsy
- only for clinical situations in which diagnosis is unclear

Describe diagnostic testing, findings and treatment of ALI:
- Category IIb: Immediately threatened
- Dopplers:
- Inaudibale arterial
- Audible venous
- Motor/Sensory function assessment:
- Mild or moderate muscle weakness
- Sensory loss more than toes and with rest pain
- slow-to-absent capillary refill
- Emergent (Class I) - salvageable if treated emergently
- Anticoagulation
- Revascularization

Define critical limb ischemia (CLI)
- chronic ( > 2 week) ischemic rest pain
- nonhealing wound/ulcers or gangrene in one or both legs
- attributable to objectively proven arterial occlusive disease

Describe the findings

- Incorrect electrode placement ( +1 )
- abrupt R-wave increase in lead V2 followed by much smaller R wave in V3
- V2 is actually V6
-
Atrial tachycardia ( +4 )
- P-waves of sinus origin should be positive in lead II
- PVC’s ( +1 )
- Inferior MI, age indeterminant or probably old ( +1 )
Describe the findings

- Atrial flutter ( +4 )
- LAD ( +1 )
- LVH ( +1 )
- RVH ( +1 )
- RBBB, incomplete ( +1 )

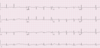
Describe the findings

- NSR ( +1 )
- LAE ( +1 )
- AV block, second degree, Mobitz I (Wenckebach) ( +4 )

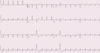
Describe the findings

- NSR ( +1 )
- AV block, second degree, Mobitz I (Wenckebach) ( +4 )
- LAD ( +1 )
- IVCD, nospecific type ( +1 )
- QRS slightly widened (approximately 115 ms) but criteria for LBBB are not met

Describe the findings

- NSR ( +1 )
-
PAC’s ( +2 )
- single dropped beat toward the end of the tracing
- T-wave preceding this dropped beat has a slightly different morphology
- PAC burried within the T wave –> dropped beat

What are the recommendations for surgery for TAA disease based on size and rate of growth of aneurysm?

What are the types of acute aortic syndromes?
- Aortic dissection
- Intramural hematoma
- Penetrating aortic ulcer
- Rapid Aneurysm expansion
- Aortic Rupture

What is the agent of choice for reversal?
- acute cerebral hemorrhage
- warfarin use
- INR 3
4F-PCC 1500 units
- contains purified vitamin K-dependent clotting factors
- do not require ABO compatibility and can be stored at room temperature
- dosing:
- INR and
- bodyweight

Describe the findings

- NSR ( +1 )
- AV junctional rhythm / tachycardia ( +1 )
- AV block, third degree ( +4 )
- Inferior MI, age recent or probably acute ( +4 )

Describe the findings

- NSR ( +1 )
- LAE ( +1 )
- AV block, second degree, Mobitz II ( +4 )
- Nonspecific ST and/or T wave abnormalities ( +1 )