What are the gastric layers? Which is strongest?

From outside to inside: Serosa - Muscle - Submucosa - Mucosa
Submucosa is the strongest (holdng layer)

Pica predisposes animals to gastric foreign bodies. Name some conditions that predispose an animal to pica.
Iron deficiency
Hepatic encephalopathy
Pancreatic exocrine insufficiency
Which of these is not a clinical sign associated with a gastric foreign body?
Vomiting
Fever
Lethargy
Abdominal pain
Anorexia
Fever
Which of these are possible lab findings for an animal with a gastric foreign body?
Anemia
Leukocytosis
Leukopenia
Neutropenia
Renal azotemia
Pre-renal azotemia
Metabolic alkalosis
Metabolic acidosis
Hyperkalemia
Hypokalemia
Hyperchloremia
Hypochloremia
Anemia
Leukocytosis
Pre-renal azotemia
Metabolic alkalosis
Metabolic acidosis
Hypokalemia
Hypochloremia
If you decide to medically manage a foreign body, what do you need to include in your therapy?
If you needed to induce vomiting, what would you use?
Fluid therapy: rehydrate, correct electrolyte imbalances
Monitor using serial rads
Induce vomiting in dog- Apomorphine
Cat- Xylazine
T/F: Many gastric foreign bodies can be removed endoscopically.
True
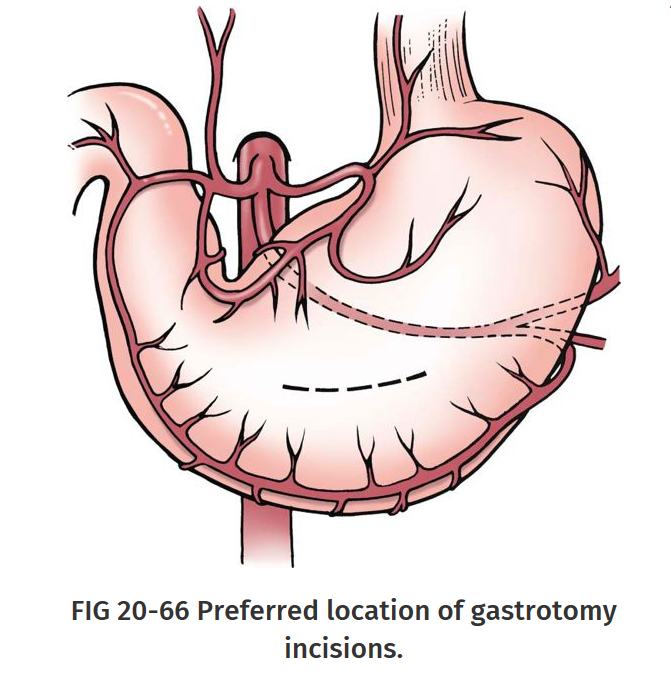
Where should you make your surgical approach for gastric foreign body removal?
Ventral midline celiotomy (from xiphoid to pubis)
Incision in hypovascular aspect of stomach between greater and lesser curvature
To reduce contamination during a gastrotomy, isolate the stomach from the remaining abdominal contents with moistened _________. Place _________ to assist in manipulation of the stomach and help prevent spillage of gastric contents.
Laparotomy sponges
Stay sutures
How do you close a gastrotomy incision- what pattern(s) could you use in the first layer and what tissue(s) will this layer incorporate? Second layer?
What alternative method could you use to reduce post-op bleeding?
First layer: Cushing or simple continuous pattern
Tissues: Serosa, muscularis, and submucosa
Second layer: Lembert/Cushing pattern
Tissues: Serosa, muscularis and submucosa
Alternative: Close mucosa in simple continuous pattern as separate layer followed by inverting pattern including all other tissue layers
(Cushing then Cushing/Lembert = Double layer inverting
Simple then another simple followed by Cushing/Lembert= Double layer appositional then inverting)
What clinical signs are associated with gastric outflow obstruction?
Chronic intermittent vomiting of partially digested food hours after feeding
(If congenital signs seen at weaning)
What congenital abnormality causes benign gastric outflow obstruction?
Pyloric stenosis
What artery supplies the lesser curvature of the stomach? What is/are the parent artery/arteries?
Greater curvature? What is/are the parent artery/arteries?
Lesser- Gastric arteries (left and right)- parent- Celiac artery
Greater- Gastroepiploic arteries (left and right)- parent = Celiac A
Short gastric arteries - parent= Splenic A

What breeds are predisposed to congenital pyloric stenosis?
Brachiocephalic dog breeds (Boxers, bulldogs)
Siamese cats
What is the suspected etiology for congenital pyloric stenosis?
Excess gastrin production
(trophic for gastric smooth muscle and mucosa)
Also possible cause of Chronic Hypertrophic Pyloric Gastropathy
What are the diagnostic modalities for determining pyloric stenosis?
Radiographs- to look for gastric distenssion or delayed gastric emptying (evidenced by a not-empty stomach after 8 or more hours of fasting)
Contrast radiography- to look for ‘beak’ or ‘apple core’ sign
Ultrasonography-
What surgeries can you perform to correct congenital pyloric stenosis?
Pyloromyotomy (Fredet-Ramstedt procedure)
Transverse pyloroplasty (Heineke-Mikulicz procedure)

Aquired hypertrophy of which layer or layers of the pyloris causes CHPG (chronic hypertrophic pyloric gastropathy)? Which breeds are predisposed? Is there a sex or age prediliction?
Mucosa and or muscular hypertrophy
Small breed dogs (<10kg) such as Shih-tse, Lhasa apso, Maltese
Males predisposed
Middle aged to older
What diagnostic tool can be used to evaluate the middle and pyloric wall thickness to diagnose CHPG? What alernative modality can you use if you also need to take biopsies?
Ultrasound
Endoscopy
In addition to a Heineke-Mikulicz pyloroplasty, which 2 other surgical techniques can you use to manage CHPG? What are advantages and disadvantages of each?
Y- U Pyroplasty
_Advantages:_Increase diameter of pylorus, access to excise hypertrophied mucosa
Disadvantages: Potential flap tip necrosis, possible side effect of rapid gastric emptying
Pylorectomy w/Gastroduedenostomy (Bilroth I)
Advantages: All diseased tissue can be removed
Disadvantages: technically more demanding, increased risk of “dumping” syndrome and reflux gastritis (due to direct connection between duodenum and stomach)

_________ tumors are commonly found near the cardia.
_________ tumors are commonly found in the pyloric antrum or the lesser cuvature of the stomach.
Leiomyoma, LSA
Adenocarcinoma
What are the sigalment, physical finding, treatment options and prognosis for gastric adenocarcinoma?
Signalment: Male, 8-10yo, Staffies, Belgian shepherds
Physical findings: plaque-like mucosal lesions with ulcers, raised sessile or polypoid lesions, diffuse infiltration (linitis plastic, scirrhous stomach wall), on US see mural thickeing and loss of normal gastric wall
Treatment options: aggresive sx exision via gastrectomy, 5cm margins
Pallitative tx: By-pass procedure (Bilroth I or II), chemotherapy?
Prognosis: Guarded to poor, no sx= 2-4mo, aggressive therapy= 10mo
What are the sigalment, physical finding, treatment options and prognosis for gastric leiomyosarcoma?
Signalment: 7-8 yo
Physical findings: ulceration, mass near cardia protruding into the gastric lumen
Treatment options: submucosal resection, Partial gastrectomy (if extensive or ulcerated)
Prognosis: median survival 21 mo, good to guarded, recurrence possible
What are the sigalment, physical finding, treatment options and prognosis for gastric leiomyoma?
Signalment:older dogs, INCIDENTAL finding
Physical findings: mass near cardia protruding into the gastric lumen
Treatment options: submucosal resection, Partial gastrectomy (if extensive)
Prognosis: Good to guarded
How would you describe this stomach wall that has been affected by a gastric adenocarcinoma?

Scirrhous





-
Wounds (E1)117
-
Ear (E1)21
-
Upper airways (E1)85
-
Kidney and Ureters (E1)46
-
Bladder and Urethra (E1)49
-
Breed Predispositions12
-
Female Repro (E1)9
-
E2: Stomach and GDV79
-
E2: Intestinal surgery (incl rectum and anus)65
-
Lab: Anesthesia Quiz65
-
E2: Hepatobilliary (incl PSS)40
-
E2: Spleen, Pancreas and Peritonitis54
-
E1: Sx Oncology22
-
E2: Dentistry and Periodontal disease113
-
E2: Oral Sx, jaw fractures and Head/neck Sx46
-
Lab: Instruments60
-
Lab: Emergency Sx, Ceilotomy, OVH, Castration72
-
Lab: Ortho exam, Bone healing28
-
Lab: Suture, Bandaging and Asepsis54
-
Final: OA/ OCD, Shoulder, Elbow90
-
Final: Hip, Stifle64
-
Final: Fracture fixation- pins, ESF, screws, plates, interlocking nails95
-
Final: Fractures62
-
Final: Hernias27
