A 23-year-old man presents with painful, red swelling over the dorsum of the right middle finger metacarpophalangeal (MCP) joint 3 days after he punched someone in the face during a bar fight. The patient reports decreasing range of motion of the hand and inability to grasp objects. He was previously seen in the emergency department the night of the injury and x-ray studies were negative for fracture or foreign body. Which of the following is the most likely causative organism?
A) Clostridium perfringens
B) Eikenella corrodens
C) Pasteurella multocida
D) Pseudomonas aeruginosa
E) Staphylococcus epidermidis
The correct response is Option B.
Eikenella corrodens is an anaerobic organism present in human oral flora and has been associated with human bite wounds. Group A Streptococcus is also a common pathogen in a fight bite injury like the one this patient has.
This patient has most likely sustained a “fight bite,” which results from tooth penetration of the metacarpophalangeal (MCP) joint after striking someone in the mouth with a clenched fist. These injuries can often be underappreciated, as the underlying defect in the extensor hood and joint capsule may not be seen on examination when the fingers are extended during examination in an emergency department. The joint can become contaminated with oral flora. Penetrating injury with high bacterial load can result in a septic joint and lead to destruction of cartilage and osteomyelitis. Recreation of the flexed fist position may help in lining up the structures and assist in identification of the injury. Treatment is aggressive antibiotic therapy and surgical exploration with irrigation and debridement of the joint to remove debris.
Clostridium perfringens is a gram-negative rod associated with gas gangrene, which results in subcutaneous crepitus and can be rapidly progressive. Pasteurella multocida is a gram-negative anaerobic bacterium most commonly associated with cat bite infections. Pseudomonas aeruginosa is a gram-negative rod that can be associated with diabetic wound infections. And Staphylococcus epidermidis is a gram-positive cocci present on the skin. It has been associated with implant infections. None of these pathogens are as likely to be present in a fight bite as Eikenella corrodens.
A 34-year-old woman comes to the emergency department 5 days after sustaining a cat bite to the left index finger. A photograph is shown. Medical history includes diabetes mellitus type 1. Physical examination shows punctures to the dorsum and volar surfaces of the proximal phalanx, mild fusiform swelling of the digit with tenderness over the flexor tendon sheath, pain with passive extension, and partially flexed posture of the digit. The symptoms have worsened over the past 3 days. Temperature is 99°F (37.2°C). Which of the following is the most appropriate next step in management?
A) Incision and drainage of the puncture sites
B) Inpatient intravenous antibiotics
C) Irrigation of the flexor sheath
D) Outpatient oral antibiotics
E) Splinting immobilization and elevation

The correct response is Option C.
The most appropriate option for this patient is to proceed to the operating room for decompression/drainage of the flexor tendon sheath. This patient has all four of Kanavel’s signs, specifically pain on passive extension, fusiform swelling, flexor tendon sheath tenderness, and flexion of the affected digit. These point towards a diagnosis of flexor tenosynovitis, with the cause being the cat bite she sustained several days prior. Although cat bites only reflect 5% of all animal bites, they represent 76% of all infected bites, thought to be because of the morphology of their long teeth, which simulate a deep puncture wound.
Outcomes studies demonstrate that because of this patient’s diabetes, she is at risk for a poor outcome, specifically the need for amputation and/or decreased total active motion. Other risk factors that can lead to these outcomes include age greater than 43 years, presence of subcutaneous purulence, digital ischemia, and polymicrobial infection. Given that she is at risk and that she has all four Kanavel’s signs, any intervention that is more conservative than operative decompression and drainage may lead to suboptimal outcomes.
Administration of antibiotics (orally or intravenously) is not a substitute for drainage of the flexor sheath, especially in a case that presents more than 48 hours out from initiation of symptoms. Drainage in the emergency department is not as optimal as in the operating room given that the infection may limit efficacy of local anesthesia as well as the need for possible conversion to an open drainage procedure if closed catheter irrigation is insufficient.

A 55-year-old man undergoes microsurgical replantation of an amputated ear. There is venous congestion, and leeches are applied. This patient is at risk for infection by which of the following organisms?
A) Actinobacillus lignieresii
B) Aeromonas hydrophila
C) Eikenella corrodens
D) Pasteurella canis
The correct response is Option B.
Aeromonas hydrophila is an organism present in the leech species Hirudo medicinalis gastrointestinal tract that can lead to an infection if used medicinally. In this patient with venous congestion and application of leeches, antibiotic prophylaxis is recommended with fluoroquinolones, tetracycline, or trimethoprim-sulfamethoxazole.
Actinobacillus lignieresii is seen in horse bites, Pasteurella canis in dog bites, and Eikenella corrodens in human bites.
In a recent review of ear reattachment methods, a variety of approaches have been used including microsurgical reattachment, burying of the part in a subcutaneous pocket, periauricular tissue flaps for coverage of the part, and direct reattachment as a composite graft. Microsurgical replantation is associated with the best aesthetic outcome even if venous anastomosis is not possible and leeching is necessary.
To drain a thenar space infection, the dissection is carried out:
A) volar to the abductor pollicis brevis muscle
B) ulnar to the vertical septum between the third metacarpal and long finger profundus tendon
C) volar to the opponens pollicis muscle
D) volar to the adductor pollicis muscle
E) volar to the flexor pollicis longus tendon
The correct answer is option D.
The dorsal border of the thenar space is the adductor fascia, hence drainage of the thenar space entails dissection volar to that muscle. The thenar space is located radial to the vertical septum between the third metacarpal and the long finger profundus and extends to the lateral edge of the adductor pollicis. The space is bounded anteriorly by the thumb and index flexor tendons, posteriorly by the fascia over the adductor pollicis, radially by the thenar intermuscular septum and ulnarly by the midpalmar oblique septum. The abductor and opponens pollicis muscles are superficial (volar) to the thenar space.

A 50-year-old man comes to the office because of a 2-day history of worsening erythema, swelling, and tenderness of the interphalangeal (IP) joint of the thumb. He reports similar episodes in the past involving other joints but does not recall any history of trauma or skin breakage in the area. X-ray study of the thumb shows soft-tissue swelling only. No bony abnormalities are noted. Which of the following is the most appropriate first step in management?
A ) Administration of antibiotics
B ) Aspiration of joint fluid
C ) Elevation and splinting of the joint
D ) MRI of the joint
E ) Surgical washout
The correct response is Option B.
The most appropriate first step in management in the scenario described is to aspirate fluid from the joint for analysis. There are several conditions that mimic acute hand infections, and it is important to recognize them so that the appropriate treatment can be initiated. Crystalline deposition diseases, such as gout and pseudogout, tend to present with joint swelling, erythema, pain with motion, and fever, much like the signs of infection. The only way to confirm the diagnosis is to aspirate the joint and look for crystals with polarizing microscopy. Though the description of the thumb in the scenario described is consistent with possible infection, the fact that there has been no trauma or break in the skin around the joint, and the patient’s history of acute arthritic episodes in other joints, raises some suspicions that this could be noninfectious. Therefore, joint aspiration to rule out other causes of acute arthritis is warranted. Administration of antibiotics and elevation and splinting should begin after the aspiration, if indicated. MRI of the joint and surgical washout are not indicated at this time.
A 41-year-old woman who is a dentist comes to the office because she has I had intense burning and pruritus of the dominant index finger for the past 6 days. The patient reports a small vesicular rash on the finger that has since progressed to form a small blister. She has had intermittent fever and malaise. Which of the following is the most appropriate management?
A) Incision and drainage of the bullae
B) Intravenous administration of cefazolin
C) Oral administration of acyclovir
D) Topical application of silver sulfadiazine
E) Observation only
The correct response is Option E.
The patient has a history and physical findings consistent with herpetic whitlow. This is a viral infection caused by herpes simplex virus and is more common in medical and dental personnel. Tzank smear or antibody titers can confirm a diagnosis but are unnecessary in the management of this patient. Treatment is primarily nonoperative and involves observation, as the course of the illness is self limiting with resolution in 1 to 3 weeks. Intravenous antibiotics would not treat this viral infection. Incision and drainage is unnecessary and may lead to a bacterial superinfection or systemic dissemination of herpes simplex virus.
Acyclovir or valacyclovir may shorten the duration of symptoms, but must be started within 2 to 3 days of onset.
Topical application of an antimicrobial would provide no benefit in this case.
Surgical drainage of the bullae should not be performed because it may increase the risk of spreading the herpes virus and may also lead to bacterial superinfection.
A 15-year-old girl has two draining nodules of axillary hidradenitis suppurativa. Each lesion is approximately 10 mm in diameter. The remaining axillary skin shows no abnormalities. After a 6-week course of oral doxycycline and topical mupirocin, the lesions drain less but are still present. Which of the following is the most appropriate treatment for this patient?
A) Complete axillary excision and skin grafting
B) Excision and closure
C) Incision and drainage
D) Intravenous antibiotics
E) Kenalog injection
The correct response is Option B.
This young patient has limited, focal disease that has failed medical management. Local excision is useful for isolated, scattered individual, or linear lesions. More extensive disease that occupies a significant portion of the skin area may be better treated by complete axillary excision. In this younger patient with limited disease, direct excision of the affected areas is a less morbid approach. Negative pressure wound therapy and skin grafts may be optimal coverage treatments for extensive disease, and some local flaps have been described as well. This stubborn disease originates from the apocrine glands and can often be chronic and disabling. The axillae, groin, perineum, and submammary areas can all be affected. Initial treatments include local care, antibiotics, hygiene, and weight loss. Steroid injections may help in early, small lesions, but have limited effectiveness and are painful. After a 6-week course of antibiotics, this patient is not likely to benefit from more treatment. Only excision of the diseased apocrine glands is likely to be effective. Incision and drainage is a suitable treatment for a closed abscess associated with hidradenitis, but incising this patient’s lesions would not improve her situation.
An otherwise healthy 27-year-old man sustains a scorpion sting on a camping trip. Which of the following is the most appropriate management?
(A) Application of cold compresses
(B) Application of a tourniquet
(C) Administration of diazepam
(D) Administration of scorpion antivenin
(E) Debridement of the affected area
The correct response is Option A.
Because scorpion stings are typically self-limiting in adults, management should be limited to observation and application of cold compresses. Six closely related species of scorpion found in the southwestern United States cause medically significant injuries resulting from a sting. These species are typically 1 to 7 cm long and yellow-brown in color, possibly with vertical bands. The venom is neurotoxic, resulting in activation of the autonomic nervous system and depolarization of the neuromuscular junctions. Affected patients have intense localized pain and hyperesthesia; there is severe pain with light tapping over the area of the wound. Other symptoms seen in patients who sustain scorpion stings include blurred or diminished vision, strabismus, dyspnea, wheezing, dysphagia, urinary or fecal incontinence, opisthotonos, fever, and involuntary muscle contractions.
Hospital admission is recommended for children who have scorpion stings because envenomation is much more dangerous than in adults. Appropriate pediatric management includes airway control, sedation, cardiac monitoring for potential arrhythmias, and administration of calcium gluconate for treatment of muscle spasms. Narcotic agents should not be administered as they may exacerbate the neurotoxic effects. Scorpion antivenin is available for use in Arizona.
The use of tourniquets is not recommended in patients with scorpion stings. Debridement is not necessary because scorpion venom has only localized adverse effects on soft tissue.
A 43-year-old healthy man comes to the office because of acute swelling over the dorsum of his dominant right wrist. He says that movement of the wrist is painful. No preceding trauma is noted. Which of the following is the most sensitive test to diagnose septic wrist arthritis in this patient?
A ) Carpal bone radiographic destructive changes
B ) Joint aspirate Gram stain
C ) Serum erythrocyte sedimentation rate
D ) Serum white cell count
E ) Synovial fluid white cell count
The correct response is Option E.
Analysis of synovial fluid is the most useful diagnostic test. The most definitive test of the joint fluid, bacterial Gram stain and culture, is unfortunately not consistently positive in an acute septic joint. Culture may be negative in about 50% of cases, especially gonococcal, and Gram stain is even less frequently positive. One has to wait a few days for culture results.
As one lowers the threshold for the white cell count in a joint aspirate, the test becomes more sensitive, but less specific. If the white cell count threshold is set at 50,000/mL, which is traditionally the value considered to be the threshold for diagnosis of a septic joint, the sensitivity is 61%. If a white cell count at 17,500 is set as the threshold, the sensitivity is 83%, but specificity is 67%. The specificity rises to 77% if the threshold for the white cell count is raised to 100,000.
Sedimentation rate, serum white cell count, and C-reactive protein do little to change pretest probability of a septic joint.
Radiographic changes are a late finding in septic arthritis.
A 67-year-old man with type 1 diabetes mellitus is evaluated for full-thickness perineal burns sustained by falling onto a space heater. Forty-eight hours after admission, he has onset of fever and tachycardia. Complete blood cell count shows leukocytosis, and wound culture was positive for gram-negative rods consistent with Pseudomonas. Pending sensitivity report, empiric coverage is initiated. Which of the following antibiotics is clinically CONTRAINDICATED for initial therapy?
A) Ceftazidime
B) Ceftriaxone
C) Ciprofloxacin
D) Imipenem
E) Tigecycline
The correct response is Option E.
Although tigecycline has excellent coverage of most staphylococcal and many gram-negative rod infections, this tetracycline derivative is not effective against pseudomonal infections. Patients with pseudomonal sepsis benefit from double coverage. Furthermore, sensitivities to different antimicrobial agents are quite variable from one health care system to another, so providers must remain vigilant after beginning therapy and change coverage based on lack of clinical response and determination of final sensitivities. An essential component of this patient’s care would be urgent burn wound excision, after he has been resuscitated and empiric antibiotics have been initiated.
A 34-year-old man has had pain and swelling of the long and ring fingers for the past three days. On physical examination, there is a sausage-like appearance of the fingers. The patient has pain on passive stretch of the fingers, and there is tenderness over the flexor tendon sheaths. Radiographs show swelling of the soft tissues.
In addition to intravenous administration of antibiotics, which of the following is the most appropriate management?
(A) Needle aspiration of the flexor tendon sheaths
(B) Incision into the fingers
(C) Incision into the joints
(D) Incision into the palm
(E) Opening and irrigation of the flexor digital sheath
The correct response is Option E.
This 34-year-old man has findings consistent with advanced flexor tenosynovitis. The diagnosis can be made by the presence of one or more of Kanavel’s four signs (fusiform swelling, partial flexed posturing of the finger, tenderness over the flexor tendon sheath, and pain with passive extension of the finger). This patient exhibits three of the diagnostic signs, indicating an advanced disease course. In addition to intravenous administration of antibiotics, the most appropriate management is opening and irrigation of the flexor tendon sheath. The surgeon should make an incision into the palm that is sufficiently wide to allow for access to and visualization of the proximal aspect of the A1 pulley. Another incision is made distally to allow access to the A4 and A5 pulleys. If necessary, the incisions can be extended distally and/or proximally to treat infected, necrotic tissue.
In patients with advanced flexor tenosynovitis, the flexor digital sheath is typically distended with purulent material. A plastic irrigation catheter is inserted at the level of the A1 pulley and threaded distally into the sheath to allow for irrigation beyond the A5 pulley. This technique will facilitate complete decompression of the sheath without sacrificing
the pulleys. Irrigation can be provided via the catheter continuously for as long as 24 hours, depending on the severity of infection.
Needle aspiration is useful in establishing a diagnosis of or treating early tenosynovitis (characterized by the presence of only one or two of Kanavel’s signs) or as initial treatment during pregnancy. Simple incision into the finger, joint, or palm will not address in the infection of the flexor tendon sheath.
A 30-year-old man with AIDS is evaluated for a 6-week history of painless but increasing swelling of the flexor surfaces of the right wrist. Physical examination shows limited motion of the wrist and positive Phalen and Tinel signs. At the time of surgical exploration, rice bodies are present in the flexor tenosynovium. Which of the following is the most likely diagnosis in this patient?
A) Aspergillus fumigatus
B) Mycobacterium tuberculosis
C) Nocardia asteroides
D) Sporothrix schenckii
E) Vibrio vulnificus
The correct response is Option B.
Rice bodies are pathognomonic for tuberculosis.
Ziehl-Neelsen staining confirms the presence of acid-fast bacilli. All Mycobacterium and Nocardia species are potentially acid-fast. Many of these organisms are fastidious, so false-negative results are common. Surgeons should obtain multiple tissue samples and alert the laboratory that a diagnosis of tuberculosis is suspected. M. tuberculosis is traditionally cultured in Löwenstein-Jensen culture medium under specific temperature conditions 37.0°C (98.6°F). Histologic examination of specimens shows a granulomatous inflammatory process with the central portion of the granulomas appearing caseated.
If a mycobacterial infection is suspected, a Mantoux test should be performed. The test involves purified protein derivative injection into the dermis and evaluation of the cutaneous site after 48 to 72 hours.
M. tuberculosis should be considered in all immunocompromised patients. The other organisms can all be seen in hand infections in immunocompromised patients but do not produce rice bodies.

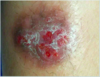
A 40-year-old woman with chronic hidradenitis suppurativa of the bilateral axillae is referred for surgical management after 4 years of local wound care, multiple corticosteroid injections, and oral antibiotics failed to improve her symptoms. Physical examination shows multiple inflamed nodules and draining sinuses. Photographs are shown. Which of the following treatment options is most likely to provide long-term resolution of this patient’s symptoms?
A) Axillary lymphadenectomy and coverage with a trapezius flap
B) Carbon dioxide laser and silver sulfadiazine
C) Fistulotomy and negative pressure wound therapy
D) Lesion excision and primary closure
E) Total axillary excision and skin grafting

The correct response is Option E.
Hidradenitis is a chronic and often disabling skin condition of the apocrine glands. It results in abscesses, inflammatory nodules, and draining sinuses in the axillae, groin, perineum, and occasionally the submammary area. It affects approximately 1 in 300 people, and it is more common in women, people who smoke, and people who are overweight. The axillae are more commonly involved in women, and the perineum more commonly in men.
Early treatment centers around local wound care, oral antibiotics, corticosteroid injections, hygiene, weight loss, and smoking cessation. Decreased estrogen levels may also contribute, and disease often subsides with oral contraceptives and during pregnancy. Unresponsive or extensive disease requires surgical intervention for long-term resolution. Relapse rates are high, and healing is often slow. Although limited excision and closure of solitary lesions is an effective short-term treatment, new lesions are likely to develop. Fistulotomy alone has an unacceptably high recurrence rate.
A long-term resolution in this severely affected patient requires complete excision of the hair-bearing skin of the affected area. The large defect created needs broad skin coverage. The best options include split-thickness skin grafting or grafting with negative pressure wound therapy immobilization. Negative pressure wound therapy followed by healing by secondary intention or coverage with local flaps are additional options, though scar contractures and shoulder stiffness are risks.
Laser treatments are too superficial to treat the deeper apocrine structures. Lymphadenectomy is not necessary for a cure.

A 40-year-old man has a painful, fluctuant abscess over the dorsal aspect of the left hand at the level of the metacarpophalangeal joints. On physical examination, the index finger is abducted away from the long finger. This abscess most likely courses through which of the following anatomic sites?
(A) Extensor tendon sheath
(B) Flexor tendon sheath
(C) Palmar bursa
(D) Palmar fascia
(E) Parona’s space
The correct response is Option D.
This patient has a collar button abscess, which communicates from the volar web space to the dorsal aspect of the hand via the palmar fascia or lumbrical canal. Finger abduction is a characteristic finding. Appropriate management is drainage of the abscess using a combined volar and dorsal approach.
The extensor tendons do not lie within sheaths on the dorsal aspect of the hand.
Infection of the flexor tendon sheath is known as flexor tenosynovitis. This condition is diagnosed by the presence of one or more of Kanavel’s signs, including fusiform swelling, partial flexed posturing of the finger, tenderness over the flexor tendon sheath, and pain with passive extension of the finger. Finger abduction is not associated.
Patients with infection of the palmar bursa have a painful prominence in the palm without finger abduction.
Parona’s space lies between the pronator quadratus and flexor digitorum profundus tendons. It communicates with the flexor tendon sheaths to the thumb and small finger (radial and ulnar palmar bursa) and the midpalmar space. Infection within this space is characterized by painful swelling over the volar aspect of the wrist that occurs proximal to the flexion crease of the distal wrist.
A 55-year-old woman has had pain, swelling, and erythema of the left arm for the past 24 hours. She underwent mastectomy and axillary lymph node dissection on the left four years ago. On examination, she is afebrile. Laboratory studies show a leukocyte count that is within normal limits.
Which of the following is the most appropriate management?
(A) Lymphatic massage
(B) Application of a compression bandage and elevation of the extremity
(C) Topical application of an antibiotic
(D) Intravenous administration of an antibiotic
(E) Incision and drainage
The correct response is Option D.
In this patient who has had the spontaneous onset of cellulitis of the arm after undergoing axillary lymph node dissection, the most appropriate management is intravenous administration of an antistreptococcal antibiotic. Fever and leukocytosis are typically associated with cellulitis but are not required to make the diagnosis, as many of these patients will be afebrile and will not have an increased leukocyte count or absolute neutrophil count on serologic testing. Anti-streptolysin O titer may be positive.
Although lymphatic massage and compression and elevation of the extremity are useful in controlling the lymphedema associated with lymph node dissection, these measures will not treat cellulitis. Antibiotic therapy should not be based on the results of blood or tissue aspirate cultures because these often do not yield any growth. Topical application of an antibiotic will not effectively treat cellulitis. Incision and drainage of the affected site is not indicated.
A 27-year-old man comes to the emergency department for evaluation after being involved in an altercation earlier in the evening during which he sustained multiple injuries to his right hand. Physical examination shows a deep laceration over his right index and long finger metacarpophalangeal (MCP) joints. There is no evidence of tendon or neurovascular injury. The wound is debrided at bedside, packed with moistened gauze, and placed in a sterile dressing. Prior to discharge, the patient should be provided with prophylactic antibiotic coverage for which of the following microorganisms?
A) Eikenella
B) Flavobacterium
C) Mycobacterium
D) Pasteurella
E) Vibrio
The correct response is Option A.
It is important to recognize dorsal hand lacerations as a possible site for serious infection, especially in the context of altercations where a “fight bite” might have occurred. In some cases, patients may be apprehensive to admit to the source of their injury, and in these cases, physicians should err on the side of caution and provide antibiotic prophylaxis. The primary bacteria isolated from human bite wounds is Eikenella. Pasteurella is commonly found in wounds resulting from the bites of dogs, cats, or farm animals. Flavobacterium is associated with bites from freshwater fish. Mycobacterium can be seen in bites from bears and ferrets. Vibrio is associated with shark bite wounds and other marine injuries.
Over the past nine months, a 58-year-old woman has had four episodes of paronychia of the right middle finger characterized by pain, swelling, and inflammation. She has taken oral antibiotics intermittently during that time; there is no purulent drainage.
Which of the following is the most likely causal organism?
(A) Candida albicans
(B) Herpes simplex virus
(C) Mycobacterium marinum
(D) Pseudomonas aeruginosa
(E) Staphylococcus aureus
The correct response is Option A.
In this patient who has a history of recurrent inflammation consistent with chronic paronychial infection, the most likely causal organism is Candida albicans, which has been shown to be responsible for as many as 97% of cases of chronic paronychia. In patients with this condition, the affected area should be kept dry and a topical antifungal agent such as clotrimazole should be applied. Eponychial marsupialization, which involves the removal of a crescent-shaped piece of skin from the eponychium, may be considered to clear the scarred, infected tissues.
Herpes simplex virus results in herpetic whitlow, an extremely painful condition characterized by visible vesicles. It is self-limiting and typically resolves in three to four weeks, but may recur. Incision and drainage are not indicated.
Mycobacterium marinum, an atypical mycobacterium, can result in superficial or deep granulomatous infections. The recommended treatment includes multidrug antituberculous therapy and surgical debulking.
Although Pseudomonas aeruginosa is part of the normal flora of the hyponychial space, this organism can result in acute infection in patients with diabetes mellitus or can be a secondary cause of chronic paronychia. Discoloration of the nail is a frequent finding.
Staphylococcus aureus is the predominant pathogen associated with acute paronychial infection, which manifests as an abscess requiring incision and drainage.
A 42-year old woman presents with a week-long history of increasing pain and swelling of her index finger PIP joint. Three weeks ago, she had sustained a puncture wound to that PIP joint in a thorn bramble. The PIP joint is mildly erythematous, moderately tender to palpation, and has 45 degrees of painful active motion. X-rays show soft-tissue swelling but are otherwise normal. You would recommend:
A) Ice and NSAIDS
B) Steroid injection
C) Incision/drainage and anti-fungal therapy
D) Physical therapy
E) Long-term cephalosporin
The correct answer is option C.
Fungal infections of the upper extremity are of four main types—cutaneous, subcutaneous, deep, and systemic. Cutaneous infections are caused by organisms capable of metabolizing keratin. The suspected organism in this case is Sporothrix schenckii. A thorn puncture is the usual mechanism of joint inoculation. Arthrotomy with synovectomy, appropriate cultures, and antifungal medication would be the best treatment. Itraconazole (100mg–200mg daily) is the preferred medication. The organism grows best at temperatures below 37°C; ice application would therefore be contraindicated. Steroid injection could potentially accelerate the infectious process. Physical therapy would not address the infection.
Cephalosporins would not be effective against a fungal infection, which would be suggested by the more subacute course of this patient.
A 53-year-old man returns to the emergency department because he has redness, swelling, and severe pain in the left upper extremity two days after he sustained a laceration to the left hand. Current temperature is 102 °F (38.9 °C) and heart rate is 126/min. Current examination shows crepitus extending into the left forearm. Radiograph shows some gas in the soft tissue. Which of the following is the most likely causative organism?
A ) Eikenella corrodens
B ) Pasteurella multocida
C ) Pseudomonas aeruginosa
D ) Staphylococcus epidermidis
E ) Streptococcus pyogenes
The correct response is Option E.
The most likely causative organism is Streptococcus pyogenes (Group A Strep).
Necrotizing soft-tissue infections (necrotizing fasciitis) are rapidly progressive and potentially lethal. Symptoms usually begin with localized erythema and swelling and may mimic cellulitis in the early stages. Severe pain, crepitus, and systemic toxicity can provide clues to the diagnosis. Radiographs may show air in the soft tissues, and patients may exhibit grayish, watery discharge (dishwater pus). These infections can be caused by polymicrobial synergistic infections or may be monobacterial in nature. A recent study showed that group A streptococcus was the most common cause of monobacterial necrotizing fasciitis and that diabetes was the most commonly associated comorbidity. Early intervention and radical debridement are key to management of necrotizing fasciitis.
Eikenella corrodens is an anaerobic organism present in human oral flora and has been associated with human bite wounds.
Pasteurella multocida is a gram-negative anaerobic bacterium most commonly associated with cat bite infections.
Pseudomonas aeruginosa is a gram-negative rod that can be associated with diabetic wound infections.
Staphylococcus epidermidis is a gram-positive coccus present on the skin. It has been associated with implant infections.
Clostridial and beta streptococcal infections are the most common causes of early-onset necrotizing infection. Diabetes mellitus is the most common morbidity.
A 45-year-old woman is referred to the office because she has had chronic infection, drainage, and pain of the left armpit for the past 10 years. The contralateral axilla is similarly affected. Medical history includes multiple courses of antibiotic therapy and intermittent drainage procedures. Physical examination shows a 10 x 15-cm area of involvement. Which of the following is the most effective management?
(A) Oral administration of an antibiotic
(B) Intravenous administration of an antibiotic
(C) Injection of botulinum toxin A
(D) Incision and drainage of the region
(E) Complete excision of the scarred area
The correct response is Option E.
Hidradenitis suppurativa is an inflammatory disease of the apocrine glands and follicular epithelium, presenting most commonly as deep recurrent infections or chronic sinus tracts in hair-bearing regions of the skin. It is most commonly seen in the axillary region in young women, but the groin and perineum may also be affected.
After the diagnosis has been confirmed, a short course of treatment with local drainage and suppressive antibiotics is appropriate. However, once the disease process is established, the only appropriate therapy is complete excision of the scarred area.
The successful treatment of chronic hidradenitis with injection of botulinum toxin A has been reported. Sweat glands have a sympathetic innervation. Botulinum toxin works by blocking the release of acetylcholine from nerve endings, thus decreasing sweat production. However, this is expensive and represents a temporary treatment of a chronic problem.
The mainstay of treatment for larger areas is complete excision of axillary skin followed by split-thickness skin grafting. Negative pressure dressings are helpful to stabilize the graft. Although numerous local fasciocutaneous pedicled and free flaps have been described, they increase the risk of donor site morbidity and are generally not necessary. Healing by secondary intention has also been described. However, it is preferable to undertake excision of one axilla at a time so the patient is not disabled in the perioperative period.
A 28-year-old, right-hand–dominant woman is brought to the emergency department 18 hours after sustaining a cat bite to the dorsum of the hand proximal to the fifth metacarpophalangeal (MCP) joint. Which of the following organisms is most likely to be cultured from this abscess?
A) Eikenella corrodens
B) Group A Streptococcus
C) Methicillin-resistant Staphylococcus aureus
D) Pasteurella multocida
E) Pseudomonas aeruginosa
The correct response is Option D.
Pasteurella multocida is a small, gram-negative coccobacillus that is frequently associated with infections caused by dog and/or cat bites. Local findings are consistent with infection including erythema, warmth, pain and tenderness, and fluctuance or purulent discharge. Delayed treatment may result in chronic deep-space infection and/or osteomyelitis. Treatment involves starting penicillin combined with local wound care as well as surgical incision and debridement if needed.
Methicillin-resistant Staphylococcus aureus (MRSA) is becoming more common in community-acquired hand infections, but is not typically associated with dog or cat bites. Eikenella corrodens is more commonly associated with infections occurring after human bites. Pseudomonas infection is often seen as a nosocomial infection that is very resistant to antibiotics. Group A Streptococcus is a common bacterial infection associated with strep throat.
A 2 year old boy is brought to the emergency department because he has had lethargy, fever, and a rash over the extremities for the past 10 hours. Temperature is 39.9C (103.8F). Physical examination shows petechiae over the trunk and arms. Over the next three hours, the rash coalesces to hemorrhagic bullae, and the diagnosis of purpura fulminans is confirmed. Each of the following management interventions is appropriate EXCEPT
(A) administration of activated protein C
(B) broad-spectrum antibiotic therapy
(C) early wound debridement and amputation of ischemic digits
(D) fasciotomy of extremities
(E) fluid resuscitation with inotropic support

The correct response is Option C.
Purpura fulminans is a frequently fatal, rapidly evolving syndrome of septic shock and hemorrhagic bullae, which can result in massive desquamation. Management includes prompt recognition of the infection (which is usually caused by Neisseria meningitidis), initiation of broad spectrum antibiotic therapy, mechanical ventilation, and aggressive fluid resuscitation with inotropic support. Disseminated intravascular coagulopathy (DIC) develops, and patients seem to benefit from replacement of activated protein C.
A recently published multicenter, retrospective review of 70 patients documented an amputation rate of 90% and suggested the need for early fasciotomy to improve limb salvage. It is difficult to determine tissue viability during the resuscitation period; therefore, debridement, coverage, and amputation are delayed until demarcation has occurred.
A 35-year-old woman with hidradenitis suppurativa and cellulitis affecting the axillae is scheduled to undergo incision and drainage and initiation of antibiotic therapy. In addition to Staphylococcus aureus, which of the following organisms is most commonly isolated in patients with hidradenitis?
(A) Peptostreptococcus sp.
(B) Pseudomonas aeruginosa
(C) Staphylococcus epidermidis
(D) Streptococcus faecalis
(E) Viridans streptococcus
The correct response is Option E.
Staphylococcus aureus and viridans streptococcus are the two most commonly isolated organisms in hidradenitis suppurativa. As a result, initial management should include empiric administration of antibiotics effective against these organisms until the results of cultures are received.
Hidradenitis suppurativa is a condition that is poorly understood but is thought to result from chronic infection of the apocrine sweat glands. Although the axillae are affected most commonly, the perineum, groin, and genitalia may also be involved. Extensive scar tissue and fistula tracts develop over time, and the condition becomes progressively more difficult to treat. In patients with hidradenitis, appropriate management is application of warm compresses, incision and drainage of the appropriate areas, and administration of antibiotics. Patients with more severe cases should undergo excision of the involved skin and subcutaneous tissue followed by coverage with a local flap or skin graft. Investigational studies of a method of immunotherapy, based on the staphylococcal phage lysate vaccine, have shown promising results in patients with chronic hidradenitis suppurativa.
A 34-year-old man is brought to the emergency department after sustaining a snake bite to the dominant right thumb. A photograph is shown above. The patient has severe pain, nausea, and vomiting. On examination, the distal forearm is tense. Prothrombin time and partial thromboplastin time are increased. The snake has been captured and was brought to the emergency department by the patient; a photograph is shown above.
Which of the following is the most appropriate management?
(A) Elevation of the extremity, application of ice, and intravenous administration of antibiotics
(B) Elevation of the extremity, application of ice, intravenous administration of antibiotics, and administration of antivenin
(C) Incision and suction drainage of the bite wound, elevation of the extremity, application of ice, and intravenous administration of antibiotics
(D) Fasciotomy and intravenous administration of antibiotics
(E) Fasciotomy, intravenous administration of antibiotics, and administration of antivenin

The correct response is Option E.
This patient who has sustained a pit viper bite to the dominant right thumb requires immediate treatment involving fasciotomy, intravenous administration of antibiotics, and administration of pit viper antivenin. Approximately 98% of venomous snake bites are from pit vipers, and more than 70% of these bites involve the upper extremity. Pit vipers can be distinguished from other snakes by the presence of two retractable maxillae, each of which contains a fang for envenomation. In patients who sustain pit viper bites, immediate first aid should consist of patient reassurance, immobilization of the affected limb and placement of the limb on a level plane, and transportation to a hospital as soon as possible. Envenomation should be assumed with the presence of fang marks and rapid swelling of the extremity; broad-spectrum antibiotics should be administered immediately in the emergency department. Patients who have tense edema of the affected extremity and compartment pressures of greater than 30 mmHg should be diagnosed with compartment syndrome. Urgent fasciotomy should be performed.
Because snake venom can greatly worsen myonecrosis and systemic findings, antivenin should be administered to any patient who has systemic symptoms of envenomation associated with increased laboratory values. Following administration of a test dose, five to 10 vials of snake antivenin are typically administered in patients who do not exhibit allergic sensitivity. A central line should be placed and emergency resuscitation should be available. The administration of as many as 20 vials of antivenin may be required in patients who have extreme abnormalities on laboratory evaluation.
Application of ice will result in vasoconstriction, ischemia, and tissue necrosis. Incision and suction drainage of the bite wound should be performed within 15 minutes of the bite.




















-
Anesthetics - Critical Care152
-
Basic Surgical Principles203
-
Blepharoplasty - Oculoplastic105
-
Body Contour - Abdominoplasty - Liposuction184
-
Breast Augmentation, Mastopexy182
-
Breast Reconstruction177
-
Breast Reduction / Gynecomastia81
-
Burns principles and treatment136
-
Chest/Abdomen/Trunk/Rec/Congenital193
-
CL & CP, CL Nose, VPI161
-
Coding27
-
Craniofacial Anomalies - Migraine212
-
Ear Reconstruction - Microtia - Trauma118
-
Oculoplastic - Eyelid Reconstruction38
-
Facelift - Browlift110
-
Facial Palsy - Cheek and Lip reconstruction77
-
Facial Rejuvenation - Chemical Peel / Fillers / Botox / Non-Surgical115
-
Facial Trauma - OMF - Mandible171
-
Flaps - Principles - Complex Flap Recons.151
-
Genital, Urinary, Gender Affirmation, Pelvic52
-
Grafts: Skin, Fat, Cartilage and Bone97
-
Hand & Lower Extremities - General75
-
Hand - Amputation, Replantation, Dupuytren's235
-
Hand - Arthritis47
-
Hand - Extensor and Flexor Tendon Injury147
-
Hand - Fractures - Dislocations77
-
Hand - Limbs - Congenital105
-
Hand Nerve Injury - Compression - Brachial plexus198
-
Hand - Tumors77
-
Hand - Wrist ligament injuries and fractures97
-
Head and Neck Anatomy - Embryology76
-
Head and Neck Congenital105
-
Head and Neck Tumors / Parotid156
-
Infections - Soft Tissue - Hand106
-
Lasers50
-
Lower Extremity218
-
Lymphedema / venous Inssuficiency43
-
Mandible - OMF93
-
Microsurgery principles51
-
Nasal Reconstruction52
-
Orthognathic, TMJ, Chin138
-
Practice management - Health Care System - Ethics - Legal - Research79
-
Pressure Injuries55
-
Rhinoplasty - Septoplasty127
-
Scalp, Forehead, Cranial Reconstruction - Hair Restoration48
-
Skin Lesions Benign, Malignant SCC BCC (No-melanoma)158
-
Skin Melanoma45
-
Tissue Expansion18
-
Wound Healing, Hypertrophic scars and Keloids, Transplant125
-
Vascular Tumors And Malformations - PAD - Trauma111
