L19: Calcium Metabolism Flashcards
(43 cards)
State some roles of calcium in body
- Muscle contraction
- Hormone secretion
- Nerve conduction
- Exocytosis
- Activation and inactivationo of many enzymes
- Intracellular second messenger (plasma to cell interior)

State some roles of phosphate in body
- ATP
- Phosphorylation and activation/deactivation of enzymes
- Hydroxyapatite crystals in mineralisation of bones
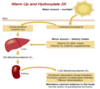
What is hydorxyapatite made of and what is it’s role?
- Calcium and phosphate
- Mineralise bone
Explain why the homeostasis of calcium and phosphate are closely linked
- Acted on by same 3 hormones: parathyroid, calcitriol and to lesser extent calcitonin
- Act on bone, kidneys and GI but often act antagonistically
Approximately how much calcium do adults contain and where is most of it stored?
1000g, 99% stored in bones in form of hydroxyapatite crystals
Roughly how much calcium is exchanged between ECF and bone each day
300-600mg
Whats the net uptake of calcium per day?
~17mg/day
~800-1200mg/day in diet but only absorb around half and then some is secreted for removal
Do the kidneys filter a large amount of calcium?
Yes, around 10x theh ECF volume. 98% is reabsorbed
State the 3 forms, and approximate proportions, calcium can exist in in the plasma
- Free ionised species (45%)
- Associated with anionic sites of serum proteins (45%)
- Complex with low molecular weight organ anions e.g. citrate (10%)
What is the total concentration (including all 3 forms) of serum calcium
What concentration is biologically active?
Total concentration: 2.2.- 2.6 mM/L
Only free ionised species is biologically active: 1.0 -1.3mM/L
Why must we monitor the calcium levels of someone who has had a large blood transfusion?
Caclium is factor IV in clotting cascade. When people donate blood we treat it with citrate as this chelates calcium ions and prevents clotting. However, if we transfuse lots of blood then we must keep an eye on their calcium levels as the citrate could chelate more calcium to lower levels
What calcium levels do labatory tests measure?
Laboratory tests measure total calcium which includes that bound to albumin and other organic anions hence a corrected level will be provided for the biologically active form
State the 3 hormones involved in calcium regulation and for each state:
- Description e.g. where made
- Effect on plasma [calcium]

How many parathyroid glands are there normally and where are they located?
4 on dorsal surface of thyroid
2.5-3% population have 6 and some have hundreds in mediastinum
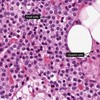
What tissue does this image show and how do you know?

Parathyroid tissue, not thyroid, as it has no follicles
Where are chief cells and oxyphil cells found; state role of each
Found in parathyroid tissue:
- Chief cells: produce and secrete PTH
- Oxyphil cells: don’t know what they do but increase in number with age

In an image of parathyroid tissue, how can you distinguish between chief cells and oxyphil cells?
Oxyphil cells fewer in number, larger and lighter staining than chief cells
How does PTH travel in blood?
On it’s own. Is a peptide hormone
Describe how chief cells respond to both low serum calcium and high serum calcium on a transcriptional level
- Low serum calcium: up-regulate gene transcription and prolong survival of mRNA of PTH
- High serum calcium: down regulate gene transcription
What is the half life of PTH?
4 mins to enable tight regulation of calcium levels. Releasd PTH is cleaved in liver
Describe why little PTH is stored
Continously made but little stored as:
- Chief cells degrade and synthesise PTH
- The cleaveage of PTH in chief cells accelerated by high serum calcium
Describe the actions of PTH on:
- Bone
- GI
- Kidneys

How does PTH act to try and reduce formation of kidney stones?
When PTH causes re-absorption of calcium it causes release of phosphate
Is vitamin D3 (activated form) a hormone?
Not technically as it isn’t secreted by an endocrine gland; it is a metabolite that acts as a hormone