L4: Lipid Transport Flashcards
(34 cards)
State 5 main classes of lipids (and any subdivision of each)

What is a phospholipid with a head group:
- Choline
- Inositol
… named?
- Choline = phosphatidylcholine
- Inositol= phosphatidylinositol
Why must lipids be transported in blood bound to a carrier? State the two most common trrasnporters.
Lipids are hydrophobic hence in soluble in water (so insolube in blood).
- 98% carried by lipoprotein particles
- 2% carried by albumin
How does our body obtain cholesterol? (2 ways)
- Most of our cholesterol synthesised by liver
- Some obtained from diet
How is cholesterol transported around the body?
As a cholesterol ester in the core/cargo & in the phospholipdid monolayer of a lipoprotein.

State three uses of cholesterol in body
- Precursor for bile salts
- Precursor for steroid hormones
- Phospholipid membranes (modulates fluidity)
Describe how cholesterol is converted into a cholesterol ester, include:
- starting products
- end products
- enzymes

(Most likely will be given this in exam but…) Estimate teh typical plasma ranges of:
- Total cholesterol
- Total lipids
… in plasma

Describe the structure of a lipoprotein, including:
- Cargo
- Surrounding monolayer
- Peripheral & interal proteins
Lipids are in NON-COVALENT association with apoproteins. They contain variable amounts of lipids.

State 3 generic roles of lipoproteins
- Transport lipids in blood
- Activate enzymes (e.g. lipoprotein lipase)
- Recognition of cell surface receptors
State the 5 lipoproteins
Fat carriers:
- Chylomicrons
- VLDL
Cholesterol ester carriers:
- IDL
- LDL
- HDL
Each contains a variable content of apolipoprotein, TAG, cholesterol & cholesterol ester
Describe and explain the stability of lipoproteins
Lipoproteins only stable if they maintain spherical shape; spherical shape is dependent on ratio of core: surface lipids. Hence, as lipids are removed from the core (by lipases or transfer proteins) lipids from surface coat must also be removed.
Describe the relationship between diameter and density of lipoproteins
Diamter is inversely proportional to density

Describe the function of each of the 5 lipoproteins (chylomicrons, VLDL, IDL, LDL & HDL)

State the 6 main classes of lipoprotein and which is most important for:
- VLDL, IDL, LDL
- HDL
Major classes: A, B, C, D, E & H
- VLDL, IDL, LDL: apoB
- HDl: apoAI
State two roles of apolipoproteins (structural & functional)
- Structural: packaging water insoluble lipids
- Functional: cofactors for enzymes & ligands for cell surface receptors
Describe how/why apolipoproteins are able to carry hydrophobic lipids in blood
Lipoproteins have phospholipid monolayer with hydrophobic tails pointing inwards (towards where main cargo lipids are carried) and hydrophilic heads pointing outwards into blood. Apoproteins also have hydrohobic and hydrophilic parts which enables them to interact with both lipids and water.
Describe chylomicron metabolism
- Pancreatic lipase hydrolyses TAGs into glycerol & fatty acids (because TAGs cannot be absorbed directly)
- Fatty acids enter epithelial cells of small intestine
- Fatty acids are then re-esterified back to TAGs using glycerols phosphate (produced from glucose metabolism)
- Packaged with other lipids (e.g. cholesterol, fat soluble vitamins) into chylomicrons. ApoB-48 is added
- Enter lymphati system, via lacteals, travelling through thoracic ducts into left sublclavian vein
- In blood, acquires apoC & apoE
- apoC binds to lipoprotein lipase on endothelial cells of capillaries in muscle & adipose tissue causing release of FA into cells
- TAG content reduced to ~20%, apoC dissociates forming chylomicron renmant
- Chylomicron returns to liver where apoE binds to LDL receptor on hepatoytes & chylomicron remnant is taken up by receptor mediated endocytosis
- Lysosomes release remaining contents for use in metabolism

For lipoprotein lipase, state:
- Role
- Cofactor required
- Where found
- Role: hydrolyses TAGs in lipoproteins
- Requires ApoC-II as a cofactor
- Found attached to surface of endothelial cells in capillaries

Describe VLDL metabolism
- VLDL made in liver (for transporting TAGs synthesised in liver to other tissue e.g. adipose tissue for storage)
- ApoB100 is added during synthesis in liver
- When VLDL enters blood, apoC & apoE are added from HDL particles
- VLDL binds to lipoprotein lipase (on surface of endothelial cells in muscle & adipose tissue) and starts to become depleted of TAGs
- In muscle, released fatty acids are taken up & used for energy production
- In adipose, released fatty acisd are used for re-synthesis of TAGs and stored as fat
- As TAG content in VLDL depletes, some VLDLs dissociated from LPL and return to liver. However, if VLDL remains bound and TAG content depletes to ~30% it becomes a short lived IDL particle
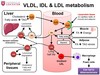
Describe IDL & LDL metabolism
IDL (made from VLDLs which have been depleted of TAGs to ~30%)
- Taken up by liver OR rebind to lipoprotein lipase to further deplete TAG content
- If TAG depletes to ~10% then apoC & apoE are lost and IDL becomes an LDL (with high cholesterol content)
- LDL can be taken up by peripheral tissues (which express LDL receptor) OR cleared by the liver (but this is inefficient as liver LDL receptor has high affinity for apoE which LDLs don’t have)
- If LDL taken up by cells, lysosomes will digest LDLs to release fatty acids & cholesterol
HOWEVER, whilst in blood, LDLs susceptible to oxidative damage and may be taken up by macrophages to form foam cells which accumulate to form a fatty streak leading to atherosclerosis.

Cells that require cholesterol will express what receptor? The expression of this receptor is controlled by what?
Cells will express LDL receptor on surface so that it can bind LDLs and then use its lysosomes to break LDLs down into fatty acids & cholesterol.
LDL receptor expression is controlled by [cholesterol] in cell e.g. if high [cholesterol] then fewer LDL receptors will be expressed
Why are LDLs more susceptible to oxidative damage than other lipoproteins?
LDLs have a longer half life in the blood hence are more susceptible to oxidative damage
State three ways in which nascent (immature) HDL particles can be synthesised
**Immature HDL particles have low TAG content
- Synthesised by liver & small intestine
- Bud off from chylomicrons & VLDLs as they are digested by lipoprotein lipase
*





