Define PE.
A consequence of thrombus formation within a deep vein of the body, embolising to pulmonary vasculature.
What is Virchow’s triad?
- stasis
- hypercoagulability
- vessel wall damage
Describe the epidemiology of PE.
Approximately 51% of DVTs will embolise to the pulmonary vasculature, resulting in a PE.
UK ~50,000 a year
1-1.5/1000 population per year
What are the risk factors for PE, relative to Virchow’s triad?
Vessel wall damage - cell damage –> thrombus formation at venous valves. Examples:
- trauma,
- previous DVT,
- surgery,
- venous harvest,
- central venous catheterisation
Venous stasis - poor flow/stasis cause thrombi and result in valvular damage, further promoting thrombus formation. Stasis increased in:
- >40yrs
- immobility
- general anaesthesia
- paralysis
- spinal cord injury
- MI, stroke,
- varicose veins,
- advanced congestive HF,
- advanced COPD
Hypercoagulability - inherited + acquired conditions:
- cancer,
- high oestrogen,
- IBD,
- nephrotic syndrome,
- sepsis,
- blood transfusion,
- inherited thrombophilia
Name 5 types of inherited thrombophilia –> hypercoagulability.
- Factor V Leiden mutation
- Prothrombin gene mutation
- Protein C and S deficiency
- Antithormbin deficiency
- Antiphospholipid antibody syndrome
Describe the consequences of pulmonary embolism on the heart.
Rarely de novo. Usually DVT –> emboli. Obstruction increases pulmonary vascular resistance (PVR) increasing the WORK or RIGHT ventricle –> increased HR (Frank-Starling). Eventually PVR is so high that there is
- over-distension of the RV
- increased RV end-diastolic pressure
- decreased RV cardiac output —> decreased LV preload –> hypotension and shock
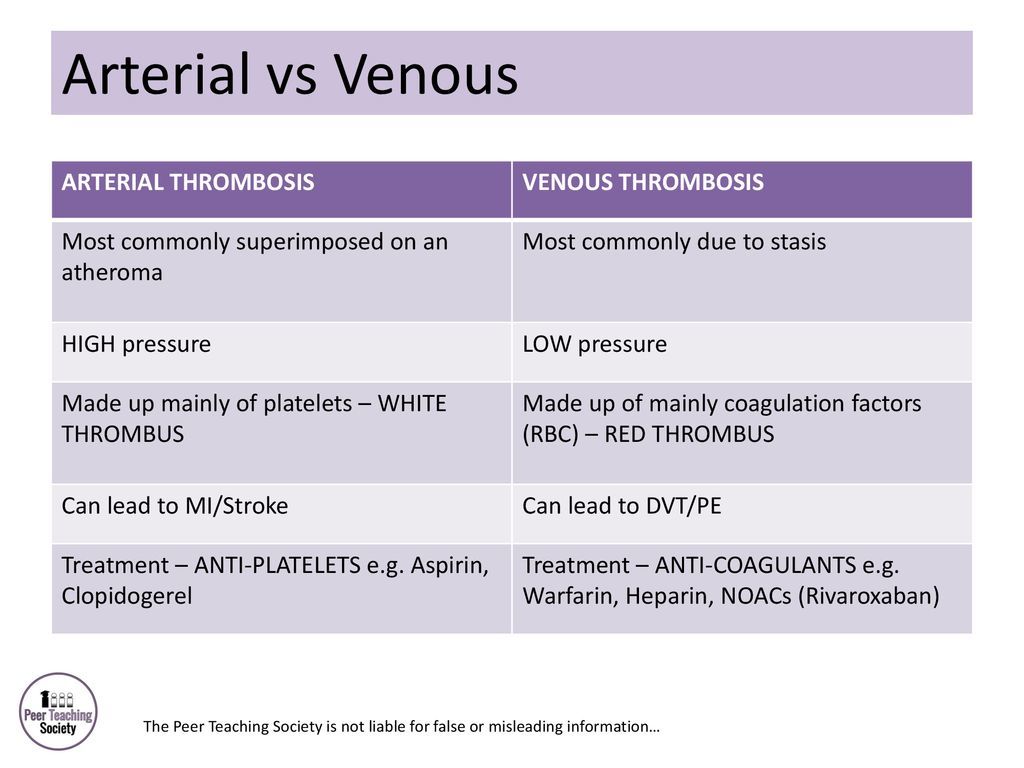
What are the differences between the thrombi formed in arteries and deep veins?
DVT = fibrin and entrapped erythrocytes (red clots). Platelet aggregation is not seen at the site of thombus attachment.
What percentage of pulmonary vasculature needs to be occluded to cause hypotension and shock?
In healthy individuals it can be as little as 50%
Symptoms of pulmonary embolism.
- Feeling of apprehension
- Cough (+haemoptysis)
- Presyncope or syncope
- Chest pain
- Dyspnoea
- Fever (in 10%)
What are the signs of pulmonary embolism on physical examination?
- Hypotension (systolic BP<90mmHg)
- Tachypnoea
- Tachycardia
- Elevated JVP (if cor pulmonale present)
- Fever
- HEAVES (sternal)
- Accentuated pulmonary component of S2 (if cor pulmonale present)
- Unilateral swelling/tenderness of calf
What initial and later investigations would you do for a PE?
History and examination, followed by 2 level Wells score to estimate clinical probability of PE.
Wells >4 then PE likely so:
- Admit
- Arrange immediate CTPA (or V/Q)
- Interim anticoagulation if delay
Wells 4 or less PE unlikely:
- D-dimer test within 4 hours
- Interim anticoagulation if delay
- CTPA if positive D dimer -
- Interim anticoagulation if delayed
- Stop anticoagulation if negative CTPA
Other tests to consider:
- Coagulation studies (INR, PT, aPTT to establish baseline)
- ABG - hypoxia and hypocapnia
- CXR
- ECG
- Lower limb USS
- V/Q scan
- Echo
- U&E
- Thrombophilia screen
- BNP, NT-proBNP, H-FABP.
What are the Wells and Geneva scoring systems?
Describe the results of these scans in PE:
CTPA
V/Q scan
Bloods:
CTPA - direct visualisation of a thrombus in pulmonary artery (partial or incomplete)
V/Q scan - an area of ventilation will not be perfused in V/Q scan
Bloods:
- Coagulation studies - establish a baseline prior to commencing anticoagulation
- U&E - guide anticoagulation
- D-dimer - ELEVATED but should not be done if the likelihood of PE is already high
What might you see in CX of pulmonary embolism? What is sometimes seen on ECG?
CXR:
- band atelectasis
- elevation of hemidiaphragm
- prominent central pulmonary artery (Fletcher’s sign)
- oligaemia at site of embolism
ECG: “S1Q3T3” pattern of acute cor pulmonale is classic; this is termed the McGinn-White Sign. A large S wave in lead I, a Q wave in lead III and an inverted T wave in lead III together indicate acute right heart strain.
Why do you give IV fluids to someone with massive PE?
Given if systolic BP is <90mmHg
How do you manage a PE?
Emergency:
- ABCDE
- Respiratory support e.g. O2
- Anticoagulation 3-6months e.g. rivaroxaban 15mg BD 3 weeks days followed by maintenance 20mg OD
Conservative:
- Monitor anticoagulation
- Provide leaflet on anticoagulation
Medical:
- Anticoagulation 3-6 months
- Thrombolysis - systemic or catheter-directed
- Open pulmonary embolectomy
Surgical:
- IVC filter -consider in those who cannot have anticoagulation
Why do you give these treatments in massive PE w/ shock/hypotension?
Vasopressors
IV fluids
IV fluids - if systolic BP is <90mmHg but aggressive volume expansion is of no benefit and may worse RV function.
Vasoactive agents (noradrenaline/dobutamine/adrenaline) - if systolic BP is less than 90mmHg then these vasopressors may be given to improve RV function and RV coronary perfusion but should be limited to hypotensive patients.
Which anticoagulants and thrombolytic therapy would you use in PE?
Offer:
1st line - apixaban or rivaroxaban
If these are not suitable: LMWH for at least 5 days followed by dabigatran or edoxaban.
Length of treatment depends on whether it is provoked or unprovoked.
What are the complications of PE and its management?
Complications:
- Acute bleeding during treatment
- Pulmonary infarction
- Cardiac arrest/death - due to acute RV failure
- Chronic thromboembolic pulmonary hypertension
- Heparin associated thrombocytopenia
- Recurrent venous thromboembolic events
What is the prognosis in PE?
- If left untreated then prognosis is poor → chronic thromboembolic pulmonary hypertension → HF
- Mortality rate is higher if patients are over 70, have cancer, CCF, COPD, systolic arterial hypotension, tachypnoea and RV hypokinesis on echo.
How can you manage cardiac arrest due to PE?
Usual CPR, adrenaline +/- defibrillation if VF/VT
Can administer thrombolysis if patient is not responding to ALS
What is the diagnosis?

Saddle PE - causing a PE on both the left and right sides.
-
Acute bronchitis11
-
Asthma21
-
Aspergillus lung disease30
-
ARDS11
-
Asbestos-related lung disease (incl. asbestosis and mesothelioma)24
-
Bronchiectasis18
-
COPD33
-
Extrinsic allergic alveoltis17
-
Idiopathic pulmonary fibrosis16
-
Lung Cancer43
-
Obstructive sleep apnoea19
-
Pleural Effusion16
-
Pneumoconiosis13
-
Pneumonia46
-
Pneumothorax26
-
Pulmonary Embolism22
-
Sarcoidosis15
-
MedEd - Chest pain38
-
Capsule Cases22
-
Procedures (chest drain)0
-
Smoking cessation4
-
Cavitating lung conditions2
-
X-rays6
