Immunodeficiency Diseases Flashcards
What do we mean by immunodeficiency?
- Infections that are…….
- O..
- U..
- Unusually …, … or not responding to … …
- F…
- Infections that are…….
- Opportunistic
- Unusual
- Unusually severe, protracted or not responding to standard therapy
- Frequent
Immunodeficiency - difficulty in defining

- So there is no definitive definition…….
- The diagnosis is largely descriptive
- Infections more likely to be significant if……..
- Infections are verified rather than simply reported
- Organisms can be identified
- End-organ damage has occurred
Infections more likely to be significant if…. (3)
- Infections are verified rather than simply reported
- Organisms can be identified
- End-organ damage has occurred
General classification of immunodeficiency
- … immunodeficiency
- … immunodeficiency …
-
Secondary immunodeficiency
- Immune defect is secondary to another disease process
- Very common
- Extremes of age
- Malignancies (esp myeloma, lymphoma)
- Metabolic eg diabetes
- Drugs eg chemotherapy, steroids
- Infection eg HIV
-
Primary immunodeficiency syndrome (PID)
- Immune defect is intrinsic to the immune system itself
- Rare
- Often genetic, but not always
- Over 100 characterised PIDS
- Mostly are fairly ‘new’ diseases
- Fatal in pre-antibiotic era
- Characterisation required developments in technology
Secondary immunodeficiency
- Immune defect is secondary to another disease process
- Very …
- Extremes of …
- … (esp myeloma, lymphoma)
- … eg diabetes
- … eg chemotherapy, steroids
- … eg HIV
- Immune defect is secondary to another disease process
- Very common
- Extremes of age
- Malignancies (esp myeloma, lymphoma)
- Metabolic eg diabetes
- Drugs eg chemotherapy, steroids
- Infection eg HIV
Primary immunodeficiency syndrome (PID)
- Immune defect is … to the immune system itself
- …
- Often …, but not always
- Over … characterised PIDS
- Mostly are fairly ‘…’ diseases
- … in pre-antibiotic era
- Characterisation required developments in …
- Immune defect is intrinsic to the immune system itself
- Rare
- Often genetic, but not always
- Over 100 characterised PIDS
- Mostly are fairly ‘new’ diseases
- Fatal in pre-antibiotic era
- Characterisation required developments in technology
Immunological classification of immunodeficiency


Immunological classification of immunodeficiency


More notes on immunodeficiency……..
- CD… T cell defects affect B cells, as T cell help is need for B cell maturation
- This is particularly marked in …; less marked in …,
- Immunodeficiency syndromes affecting both antibody production and T cells are called … …
- In addition to infections, many immunodeficiency syndromes manifest with immune …: uncontrolled …, … diseases
- CD4 T cell defects affect B cells, as T cell help is need for B cell maturation
- This is particularly marked in infants; less marked in adults, who have already matured their B cells
- Immunodeficiency syndromes affecting both antibody production and T cells are called combined immunodeficiencies
- In addition to infections, many immunodeficiency syndromes manifest with immune dysregulation: uncontrolled inflammation, autoimmune diseases
More notes on immunodeficiency……..
- CD4 T cell defects affect B cells, as T cell help is need for B cell …
- This is particularly marked in infants; less marked in adults, who have already … their B cells
- Immunodeficiency syndromes affecting both … production and T cells are called combined immunodeficiencies
- In addition to infections, many immunodeficiency syndromes manifest with immune dysregulation: … inflammation, autoimmune diseases
- CD4 T cell defects affect B cells, as T cell help is need for B cell maturation
- This is particularly marked in infants; less marked in adults, who have already matured their B cells
- Immunodeficiency syndromes affecting both antibody production and T cells are called combined immunodeficiencies
- In addition to infections, many immunodeficiency syndromes manifest with immune dysregulation: uncontrolled inflammation, autoimmune diseases
Aging and immunity (‘immunosenscence’)
‘A combination of age-related changes in the immune system that result in greater … to infection and reduced response to …’
‘A combination of age-related changes in the immune system that result in greater susceptibility to infection and reduced response to vaccination’
What is ‘immunosenscence’?
‘A combination of age-related changes in the immune system that result in greater susceptibility to infection and reduced response to vaccination’
Some immunological aspects of immunosenescence
- Thymic …
- Telomere … in stem cells reduces both quality and quantity of leucocyte output
- Reduced T and B cell receptor …
- Reduced … responses
- Reduced neutrophil function
- Reduced self-tolerance; inflammation switches from protection to damage
- Expansion of T cell pool responding to cytomegalovirus (current research focus)
- Thymic involution
- Telomere shortening in stem cells reduces both quality and quantity of leucocyte output
- Reduced T and B cell receptor diversity
- Reduced vaccine responses
- Reduced neutrophil function
- Reduced self-tolerance; inflammation switches from protection to damage
- Expansion of T cell pool responding to cytomegalovirus (current research focus)
Some immunological aspects of immunosenescence
- Thymic involution
- Telomere shortening in stem cells reduces both quality and quantity of leucocyte output
- Reduced T and B cell receptor diversity
- Reduced vaccine responses
- Reduced … function
- Reduced …-…; inflammation switches from protection to damage
- Expansion of T cell pool responding to … (current research focus)
- Thymic involution
- Telomere shortening in stem cells reduces both quality and quantity of leucocyte output
- Reduced T and B cell receptor diversity
- Reduced vaccine responses
- Reduced neutrophil function
- Reduced self-tolerance; inflammation switches from protection to damage
- Expansion of T cell pool responding to cytomegalovirus (current research focus)
Elderly clearly more susceptible to infection, but immunity itself is not the only factor:
- Reduced …
- n…
- … healing
- Co-… (COPD, CCF, DM, cancer, depression etc)
- Reduced … reserve
- All of these increase … of infection AND risk of poor … from infection
- See VZV immunisation slides: clear that older people can make a response to a specifically tailored immune booster
- Reduced mobility
- Nutrition
- Wound healing
- Co-morbidities (COPD, CCF, DM, cancer, depression etc)
- Reduced physiological reserve
- All of these increase risk of infection AND risk of poor outcome from infection
- See VZV immunisation slides: clear that older people can make a response to a specifically tailored immune booster
Predominantly antibody deficiency
- Low Ig…; other isotypes may be affected, but low IgA/ M with normal … is rarely significant
- Manifests with recurrent … infections of the upper and lower respiratory tract
- Sometimes … infections in addition
- Infections typically respond to anti-…, but response may be sub-optimal and long courses required
- If untreated, leads to irreversible lung damage (…)
- Low IgG; other isotypes may be affected, but low IgA/ M with normal IgG is rarely significant
- Manifests with recurrent pyogenic infections of the upper and lower respiratory tract
- Sometimes gut infections in addition
- Infections typically respond to anti-microbials, but response may be sub-optimal and long courses required
- If untreated, leads to irreversible lung damage (bronchiectasis)
Predominantly antibody deficiency
- Low IgG; other isotypes may be affected, but low IgA/ M with normal IgG is rarely significant
- Manifests with … pyogenic infections of the …and … … tract
- Sometimes gut infections in addition
- Infections typically respond to anti-microbials, but response may be …-optimal and … courses required
- If untreated, leads to … lung damage (bronchiectasis)
- Low IgG; other isotypes may be affected, but low IgA/ M with normal IgG is rarely significant
- Manifests with recurrent pyogenic infections of the upper and lower respiratory tract
- Sometimes gut infections in addition
- Infections typically respond to anti-microbials, but response may be sub-optimal and long courses required
- If untreated, leads to irreversible lung damage (bronchiectasis)
What is shown here?

Irreversible lung damage (bronchiectasis) as a result of untreated predominantly antibody deficiency
What is shown here?

Irreversible lung damage (bronchiectasis) as a result of untreated predominantly antibody deficiency
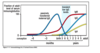
Maturation of antibody production
- In healthy infants there is normally a period of relative antibody deficiency around 6 months known as ‘transient … of infancy; this is a physiological state but can be correlated with increased …
- Infants with antibody deficiency usually present after 3-6 months; up until this time they are protected by … IgG antibody
- In healthy infants there is normally a period of relative antibody deficiency around 6 months known as ‘transient hypogammaglobulinemia of infancy; this is a physiological state but can be correlated with increased infections
- Infants with antibody deficiency usually present after 3-6 months; up until this time they are protected by maternal IgG antibody

Maturation of antibody production
- In healthy infants there is normally a period of relative antibody deficiency around 6 months known as ‘… hypogammaglobulinemia of infancy; this is a … state but can be correlated with increased infections
- Infants with antibody deficiency usually present after …-… months; up until this time they are protected by maternal IgG antibody
- In healthy infants there is normally a period of relative antibody deficiency around 6 months known as ‘transient hypogammaglobulinemia of infancy; this is a physiological state but can be correlated with increased infections
- Infants with antibody deficiency usually present after 3-6 months; up until this time they are protected by maternal IgG antibody
XLA – a prototype antibody deficiency syndrome
- Signalling via Bruton’s tyrosine kinase (btk) required for signal … at pro-… stage
- … arrest occurs if absent: no … chain rearrangement, no B cells leave marrow, no immunoglobulin production
- Disease is called …-linked agammaglobulinaemia (XLA); also known as Bruton’s disease, Btk deficiency or Bruton’s XLA
- Signalling via Bruton’s tyrosine kinase (btk) required for signal transduction at pro-B stage
- Maturation arrest occurs if absent: no heavy chain rearrangement, no B cells leave marrow, no immunoglobulin production
- Disease is called X-linked agammaglobulinaemia (XLA); also known as Bruton’s disease, Btk deficiency or Bruton’s XLA

XLA – a prototype antibody deficiency syndrome
- Signalling via Bruton’s … kinase (btk) required for … transduction at pro-B stage
- Maturation arrest occurs if absent: no heavy chain rearrangement, no B cells leave …, no … production
- Disease is called X-linked agammaglobulinaemia (XLA); also known as Bruton’s disease, Btk deficiency or Bruton’s XLA
- Signalling via Bruton’s tyrosine kinase (btk) required for signal transduction at pro-B stage
- Maturation arrest occurs if absent: no heavy chain rearrangement, no B cells leave marrow, no immunoglobulin production
- Disease is called X-linked agammaglobulinaemia (XLA); also known as Bruton’s disease, Btk deficiency or Bruton’s XLA

X-Linked hyper IgM syndrome (CD40L deficiency)
- Failure of B cell … from primary to secondary
- Low IgG & IgA, raised (or normal) Ig…
- Recurrent … infections
- Presents age 3-6 months
- The immunological … actually resides on the T cell
- CD40 ligand (also known as CD154)
- Interaction with CD40 on B cells required for affinity maturation
- Failure of B cell maturation from primary to secondary
- Low IgG & IgA, raised (or normal) IgM
- Recurrent bacterial infections
- Presents age 3-6 months
- The immunological lesion actually resides on the T cell
- CD40 ligand (also known as CD154)
- Interaction with CD40 on B cells required for affinity maturation

X-Linked hyper IgM syndrome (CD40L deficiency)
- Failure of B cell maturation from … to …
- Low Ig… & Ig…, raised (or normal) IgM
- Recurrent bacterial infections
- Presents age ..-.. months
- The immunological lesion actually resides on the T cell
- CD40 ligand (also known as CD154)
- Interaction with CD40 on B cells required for … maturation
- Failure of B cell maturation from primary to secondary
- Low IgG & IgA, raised (or normal) IgM
- Recurrent bacterial infections
- Presents age 3-6 months
- The immunological lesion actually resides on the T cell
- CD40 ligand (also known as CD154)
- Interaction with CD40 on B cells required for affinity maturation

Treating antibody deficiency
- Early recognition before … damage occurs
- Aggressive treatment of intercurrent …
- Replace …
- Long-term suppressive anti-…
- Early recognition before lung damage occurs
- Aggressive treatment of intercurrent infections
- Replace immunoglobulin
- Long-term suppressive anti-microbials

X-Linked Hyper-IgM syndrome


Cellular immunodeficiency
- Poor terminology; used to mean CD4 T cell deficiency
- When …, antibodies will also be affected (combined immunodeficiency)
- Manifests particularly with:
- … infection
- … infection
- … infection
- … infection
- Classic secondary cause is … infection
- Poor terminology; used to mean CD4 T cell deficiency
- When congenital, antibodies will also be affected (combined immunodeficiency)
- Manifests particularly with:
- Opportunistic infection
- Viral infection
- Fungal infection
- Mycobacterial infection
- Classic secondary cause is HIV infection

Cellular immunodeficiency
- Poor terminology; used to mean CD4 T cell deficiency
- When congenital, antibodies will also be affected (… immunodeficiency)
- Manifests particularly with:
- … infection
- Viral infection
- … infection
- Mycobacterial infection
- Classic … cause is HIV infection
- Poor terminology; used to mean CD4 T cell deficiency
- When congenital, antibodies will also be affected (combined immunodeficiency)
- Manifests particularly with:
- Opportunistic infection
- Viral infection
- Fungal infection
- Mycobacterial infection
- Classic secondary cause is HIV infection

Some conditions seen in cellular immunodeficiency, particularly advanced HIV

- Top left hand - candida oesophagitis
- Right hand - Cytomegalovirus retinitis
- Bottom left - Kapsosi’s sarcoma (malignancy) - driven by Human herpes virus infection
- Middle - pneumocystis carinii pneumonia (bilateral pneumonitis)
- Bottom right - compression of brain tissue - cerebral toxoplasmosis
Severe combined immunodeficiency
- …, life-threatening … immunodeficiency
- Absent … cells
- … cells may be present, but are non-functional
- All basically present in a similar fashion
- Usually soon after …
- … (graft versus host - maternal lymphocyte engraftment)
- Failure to thrive
- Chronic diarrhoea
- Infections, especially opportunistic
- Bacterial
- Mycobacterial (esp BCG)
- Viral (esp CMV, EBV)
- Fungal (PCP, oral thrush)
- Rare, life-threatening primary immunodeficiency
- Absent T cells
- B cells may be present, but are non-functional
- All basically present in a similar fashion
- Usually soon after birth
- Rash (graft versus host - maternal lymphocyte engraftment)
- Failure to thrive
- Chronic diarrhoea
- Infections, especially opportunistic
- Bacterial
- Mycobacterial (esp BCG)
- Viral (esp CMV, EBV)
- Fungal (PCP, oral thrush)

Severe combined immunodeficiency
- Rare, …-… primary immunodeficiency
- Absent T cells
- B cells may be present, but are …-…
- All basically present in a similar fashion
- Usually soon after birth
- Rash (graft versus host - maternal lymphocyte engraftment)
- Failure to …
- Chronic …
- Infections, especially …
- Bacterial
- … (esp BCG)
- … (esp CMV, EBV)
- … (PCP, oral thrush)
- Rare, life-threatening primary immunodeficiency
- Absent T cells
- B cells may be present, but are non-functional
- All basically present in a similar fashion
- Usually soon after birth
- Rash (graft versus host - maternal lymphocyte engraftment)
- Failure to thrive
- Chronic diarrhoea
- Infections, especially opportunistic
- Bacterial
- Mycobacterial (esp BCG)
- Viral (esp CMV, EBV)
- Fungal (PCP, oral thrush)

Common gamma chain deficiency and JAK3 deficiency
- Common gamma-chain deficiency
- …-linked SCID
- Common gamma chain forms part of membrane receptor for several …, some of which are required for … cell maturation
- Absent …cells
- … cells present but non-functional
- JAK-3 deficiency deficiency
- Autosomal … SCID
- JAK-3 is downstream of common gamma chain; deficiency likewise prevents signalling
- Immunologically … to gamma chain deficiency
- Common gamma-chain deficiency
- X-linked SCID
- Common gamma chain forms part of membrane receptor for several cytokines, some of which are required for T cell maturation
- Absent T cells
- B cells present but non-functional
- JAK-3 deficiency deficiency
- Autosomal recessive SCID
- JAK-3 is downstream of common gamma chain; deficiency likewise prevents signalling
- Immunologically identical to gamma chain deficiency

SCID therapy
- What is no longer used?
- Now:
- … … transplant
- .. … harvested from …-matched donor:
- Given to recipient by …
- Engraft in … …
- … of T and B cells
- Treatable - bubbles no longer used
- Stem cell transplant
- Stem cells harvested from HLA-matched donor:
- Given to recipient by infusion
- Engraft in bone marrow
- RECONSTITUTION of T and B cells

Terminal complement deficiency
- Deficiency of terminal complement components …-… leads to specific susceptibility to … Species
- Otherwise immunologically robust
- Diagnose by functional complement … (speak to your immunology laboratory)
- Deficiency of terminal complement components C5-C9 leads to specific susceptibility to Neisseria Species
- Otherwise immunologically robust
- Diagnose by functional complement assays (speak to your immunology laboratory)

Terminal complement deficiency
- Deficiency of terminal complement components C5-C9 leads to specific susceptibility to … Species
- Otherwise immunologically robust
- Diagnose by functional … assays (speak to your immunology laboratory)
- Deficiency of terminal complement components C5-C9 leads to specific susceptibility to Neisseria Species
- Otherwise immunologically robust
- Diagnose by functional complement assays (speak to your immunology laboratory)
