Define chronic rhinosinusitis (CRS).
Define chronic rhinosinusitis (CRS).
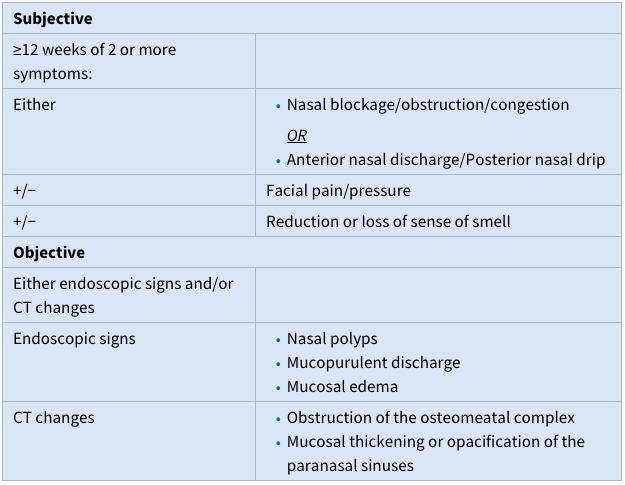
CRS is chronic inflammation of the mucosal lining of the paranasal sinuses that persists for at least 12 weeks. Clinically, rhinosinusitis is defined by clinical symptoms (subjective) plus suggestive endoscopic and/or CT changes (objective)
What are the symptoms associated with CRS in adults and children?
What are the symptoms associated with CRS in adults and children?
The most common symptoms include nasal congestion or blockage, nasal discharge (either anterior or posterior), facial pain and pressure, and reduction in sense of smell.
Other symptoms that may be associated are cough, headache, throat discomfort, laryngeal irritation, hoarseness, halitosis, ear pressure, dental pain, and malaise. In general, the same symptoms are seen with acute and chronic rhinosinusitis, but the symptom pattern and chronicity are different.

What are the endoscopic and CT findings that are typical with CRS?
What are the endoscopic and CT findings that are typical with CRS?
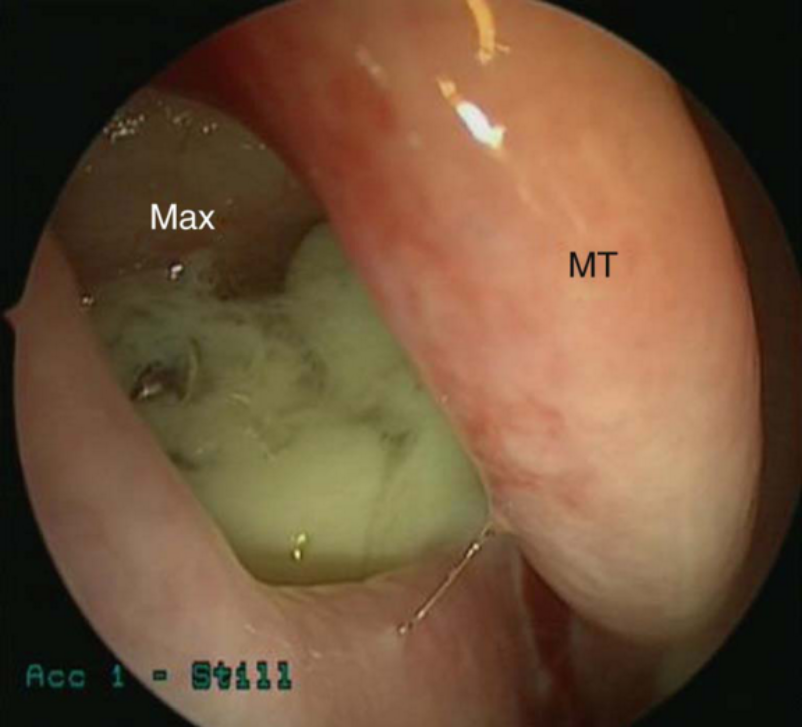
Endoscopic signs include nasal polyps , mucopurulent discharge (primarily from the middle meatus), and mucosal edema (also primarily in the middle meatus). CT findings include mucosal thickening of the paranasal sinuses and osteomeatal complex and fluid or debris in the paranasal sinuses (opacification).

How is CRS diagnosed in adults?
How is CRS diagnosed in adults?
As stated earlier, the diagnosis of CRS is based on both subjective and objective criteria.
How is CRS diagnosed in children?
How is CRS diagnosed in children?
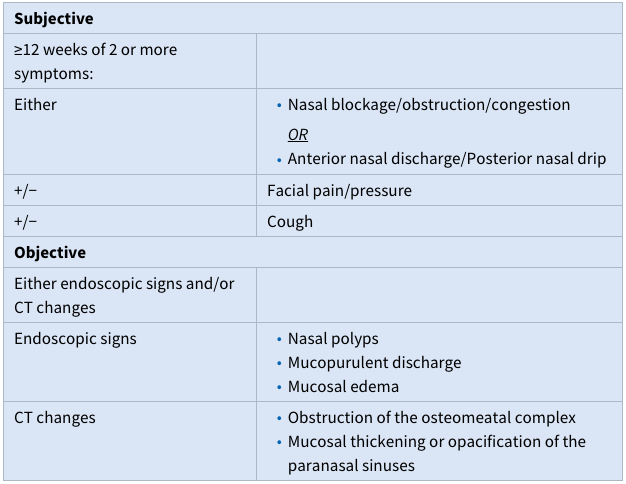
The diagnostic criteria in children are very similar to criteria in adults, however, cough is accepted as a symptom of CRS in the pediatric population. In addition, CT scans are ordered less frequently due to concern for unnecessary radiation exposure.
How common is CRS?
How common is CRS?
Based on a National Health Interview Survery, about 13% of the U.S. population report that they suffer from “sinusitis.” However, it has been shown that the incidence of physician-diagnosed CRS is only about 1% of the population. Therefore, many patients have symptoms they attribute to CRS, which are actually due to other causes, most commonly allergic rhinitis and chronic headaches. CRS has a significant negative quality of life impact, as patients report higher measures of bodily pain and lower social functioning than patients with chronic back pain, COPD, and CHF.
Describe the pathophysiology of CRS.
Describe the pathophysiology of CRS.
The cause of CRS continues to be a topic of much research and debate; however, in general it is a multifactorial inflammatory process characterized by a dysfunctional local host–environment interaction. Possible contributing factors include:
- Abnormal host production of pro- and anti-inflammatory cytokines (as is seen with nasal polyps)
- Eosinophilic tissue infiltration
- Defects in sinonasal epithelial mechanical barrier or immune response
- Defects in ciliary function
- Allergies
- Asthma
- Genetic factors may also be important and include primary immunodeficiencies and cystic fibrosis.
The role of bacteria in the development of CRS continues to be unclear, but it is widely accepted that bacteria do contribute to initiation or propagation of the inflammatory response in some way. The makeup of the bacterial community (microbiome), biofilm production, presence of intracellular or intramucosal bacteria, and Staphylococcal superantigens are all currently being studied to determine their association with CRS. It is now believed that bacteria likely are an important disease modifier.
Perhaps the two most important potential triggers underlying sinusitis are upper respiratory viral infection and upper airway inflammation from other causes. These factors may include allergy (atopy), environmental hypersensitivities, mucociliary dysfunction (primary and acquired), anatomic relationships (septal deviation, nasal polyposis), immunodeficiencies, and fungal hypersensitivities. In general, the end result of this inflammatory process is mucosal edema. Similar to acute sinusitis, this may lead to obstruction of the drainage routes of the sinuses, causing stasis of secretions and an overall physiologic change in the sinus cavity.
Which sinus is most often involved in CRS?
Which sinus is most often involved in CRS?
In contrast to acute sinusitis, the anterior ethmoid sinuses are the most commonly affected in CRS, followed by maxillary, posterior ethmoid, sphenoid, and then frontal sinuses.
What inflammatory pathways are characteristic of CRS?
What inflammatory pathways are characteristic of CRS?
There are multiple inflammatory markers that are characteristic of CRS. In general, CRS with nasal polyps (CRSwNP) is separated from CRS without NP (CRSsNP) in terms of inflammatory pathways; however, both show an *increase in proinflammatory leukotrienes_ and a _decrease in anti-inflammatory prostaglandins*.
- CRSwNP is characterized by an increase in serum and tissue eosinophilia and the Th2-mediated pathway (including IL-4, IL-5, and IL-13)
- CRSsNP is characterized by a predominance of Th1-mediated pathway, fibrosis, and high levels of TGF-β.
Those patients with asthma have increased tissue eosinophilia and predominance of Th2-mediated inflammation similar to those with CRSwNP. It appears, however, that eosinophilic inflammation is important in most forms of CRS.
Which organisms are associated with CRS?
Which organisms are associated with CRS?
The same organisms found in acute disease are also prevalent in CRS, but coagulase-negative Staphylococcus species, S. aureus, Pseudomonas aeruginosa, gram-negative rods, and anaerobes are more frequently associated with CRS. Generally speaking, gram-negative rods and staphylococcal species become more important pathogens in CRS.
What is the relationship between allergy and CRS?
What is the relationship between allergy and CRS?
Atopy and allergies lead to the elaboration of multiple early- and late-phase inflammatory mediators, many of which are also active in CRS. Theoretically, active allergies would contribute to nasal inflammation and therefore could be a disease modifier in CRS; however, this has been extensively studied and only about half of these studies have been able to find an association between the two. Therefore, the role of allergy in CRS remains controversial and not completely defined. In general, patients with allergy symptoms should be tested and treated and this can also be considered for those with recalcitrant CRS.
How does fungus play a role in CRS?
How does fungus play a role in CRS?
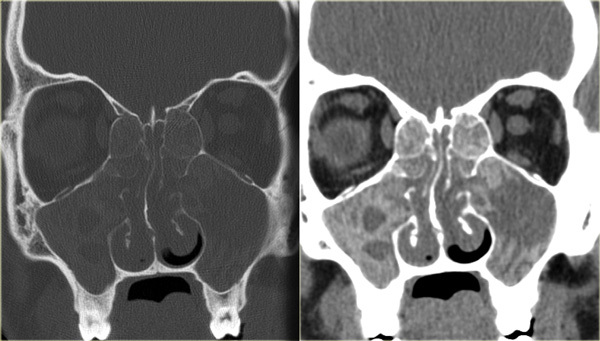
The role of fungus in CRS continues to be an area of active research. Allergic fungal rhinosinusitis (AFRS) and fungus ball (mycetoma) represent two subsets of CRS in which fungus plays a role. Both are found in immunocompetent patients in contrast to acute invasive fungal sinusitis. Diagnostic criteria of AFRS include:
- Nasal polyposis
- CT scan with evidence of hyperdense sinus infiltrates or calcifications, see figure attached.
- Eosinophilic mucin
- Noninvasive fungal identification by culture or histopathology.
These patients tend to have significant burden of polyps and over a prolonged period of time the thick, eosinophilic mucin can act as a benign soft tissue denisty in the paranasal sinuses with possible expansion into nearby structures, including the orbit and cranium. Treatment is with a combination of medical and surgical therapy, similar to other cases of chronic sinusitis. Neither systemic or topical antifungal therapy has been shown to improve treatment outcomes in this population.
A fungus ball (mycetoma) is a collection of inspissated fungal debris and mucus in an isolated paranasal sinus. Symptoms are similar to CRS or patients can occasionally be asymptomatic. The maxillary sinus is the most common location. Characteristic CT appearance is a heterogeneous hyperdensity within a sinus with microcalcifications. Intraoperatively, fungal balls appearing as a mass of thick, crumbly debris and fungal hyphae are often appreciable. Treatment is endoscopic removal, and antifungal medications are not typically required.
What is the association of asthma with CRS?
What is the association of asthma with CRS?
As the upper and lower airways (nose and bronchi) are connected anatomically and both lined by pseudo-stratified respiratory epithelium, they are often affected by similar disease processes and this is seen specifically in CRS and asthma. Asthma is present in up to 50% of patients with CRS without nasal polyps; this figure rises to 80% in the setting of CRS with nasal polyps. Both diseases can have similar inflammatory pathways, specifically eosinophilia and Th2-mediated inflammation. In general, aggressive management of CRS improves asthma symptoms. This association has lead to the “single airway” concept for this patient group.
What is aspirin exacerbated respiratory disease (AERD)?
What is aspirin exacerbated respiratory disease (AERD)?
Aspirin exacerbated respiratory disease (AERD) is a subset of CRS characterized by nasal polyps, aspirin sensitivity, asthma, and eosinophilic CRS. Previously known as Samter’s triad, AERD is now the more accepted term for this important condition. This triad, or more accurately tetrad, is present in approximately 10% to 25% of patients with CRSwNP and 25% to 40% of patients with CRSwNP and asthma. These patients are thought to have a dysfunction in the arachidonic acid metabolism pathway, with a resultant increase in the proinflammatory leukotrienes and a decrease in the anti-inflammatory prostaglandins both in serum and respiratory mucosa. Bronchospasm, mucosal edema, and an influx of eosinophils results when exposed to aspirin or nonsteroidal anti-inflammatory medications. These patients also tend to have more severe polyposis than others with CRSwNP. In addition to standard treatment for CRSwNP, aspirin desensitization is often a therapeutic option.
What is cystic fibrosis and how is it associated with CRS?
What is cystic fibrosis and how is it associated with CRS?
Cystic fibrosis (CF) is an autosomal recessive genetic disorder of the cystic fibrosis transmembrane regulator gene (CFTR). A defective chloride channel results in thick secretions and impaired mucociliary function. Manifestations include chronic pulmonary disease, pancreatic insufficiency, and CRS (with or without NPs). CF patients often have severe sinus disease requiring multiple surgeries and maximal medical therapy. Exacerbations of lung and sinus disease are often concurrent and similar to asthma. Treatment of sinus exacerbation (including surgery) can improve lung symptoms. CRS can be the presenting symptom in some patients who are heterozygous for a CFTR mutation.
How does the management of CRS differ from the management of ABRS?
How does the management of CRS differ from the management of ABRS?
The medical management of CRS differs from ABRS in that (1) the role of chronic inflammation is greater, (2) the bacterial pathogens may differ, and (3) the duration of therapy is typically longer. In addition, surgical management is a consideration in select cases of CRS refractory to medical treatment.
Discuss the role of anti-inflammatory agents in the treatment of CRS.
Discuss the role of anti-inflammatory agents in the treatment of CRS.
The majority of medical management of CRS is directed at controlling the inflammatory componet of the disease and is often more important than antimicrobial treatment. Key treatment options include nasal saline rinses, prolonged intranasal steroids, systemic steroids, leukotriene modifiers, asthma management, and immunotherapy for allergic disease. The length and type of therapy will depend on clinical symptoms and objective findings, stage of disease, and suspected underlying triggers.
Describe the role of antimicrobial treatment in CRS.
Describe the role of antimicrobial treatment in CRS.
The incidence of S. aureaus, Staph epidermidis, P. aeruginosa, and other gram-negative organisms appears to be higher in CRS than in ABRS. This presents a problem in many cases due to reduced antibiotic sensitivities for these organisms. The end result may be a limited number of oral antibiotic options, potentially increasing the need for alternative delivery options (e.g. topical). in cases where bacterial infection is suspected to be a major factor, the typical approach will be culture-directed antibiotic theraoy for a period of 3 to 6 weeks. Duration of therapy will be dependent on the patient symptoms, repeat culture data, nasal endoscopy, and CT findings. There is little current evidence, unfortunately, defining or supporting the routine use of antibiotics in the treatment of CRS. The precise role of bacteria in CRS remains poorly defined.
What is the role of surgical intervention in CRS?
What is the role of surgical intervention in CRS?
Surgery is a key component and an important consideration in the comprehensive management of CRS. Endoscopic sinus surgery (ESS) is indicated for disease that is unresponsive to medical management. The goal of surgery is to facilitate the natural drainage of the sinuses, eradicate pathogenic bacteria, and remove nasal polyps or other mucosal disease. Generally speaking, surgery is not a cure for CRS but an adjunctive treatment option for select patients. Medical management remains the primary option and is effective in the majority of patients. Recent outcomes data has demonstrated significant improvement in CRS patients that underwent ESS following failed medical therapy. In fact, data showed greater improvement in the surgical group when compared to a patient cohort that continued with medical therapy.
-
1 General Anatomy, Embryology, Radiology12
-
2 ENT Emergencies25
-
3 Deep Neck Infections27
-
9 Head and Neck Anatomy & Embryology with Radiology Correlates16
-
10 Tumor Biology22
-
11 Skin Cancer26
-
12 Diseases of Oral Cavity and Oropharynx25
-
13 Cancer of the Hypopharynx, Larynx, and Esophagus21
-
4 Antimicrobials & Pharmacotherapy17
-
5 Snoring & Obstructive Sleep Apnea26
-
6 Granulomatous & Autoimmune Disease of the Head and Neck22
-
7 Facial Pain & Headache22
-
8 Taste & Smell25
-
14 Disease of the Salivary Glands22
-
15a Disease of the Thyroid Gland32
-
15b Disease of the Parathyroid Gland14
-
16 Neck Dissection26
-
17 Vascular Tumors of the Head & Neck20
-
18 Sinonasal Tumors29
-
19 Skull Base Surgery36
-
20 Hematologic Malignancy17
-
21 Radiation & Systemic Therapy for Head & Neck Cancer27
-
22 Sinonasal Anatomy & Embryology with Radiology Correlates28
-
23 Epistaxis24
-
24 Rhinitis22
-
25 Acute Rhinosinusitis & Infectious Complications19
-
26 Chronic Rhinosinusitis19
-
27 Septoplasty & Turbinate Surgery30
-
28 Functional Endoscopic Surgery21
-
29 Cerebrospinal Fluid Leaks & Encephaloceles17
-
30 Orbital Surgery22
-
31 Otology Anatomy and Embryology with Radiology Correlates29
-
32 Hearing Loss & Ototoxicity30
-
33 Evaluation of Hearing30
-
34 TInnitus30
-
35 Evaluation of the Vestibular System & Vestibular Disorders22
-
36 Hearing Aids & Implantable Devices25
-
37 Infections of the Ear23
-
38 Complications of Otitis Media20
-
39 Tympanomastoidectomy and Ossicular Chain Reconstruction20
-
40 Otosclerosis19
-
41 Cholesteatoma18
-
42 Facial Nerve26
-
43 Surgery for Vertigo19
-
44 Neurotology29
-
45 Temporal Bone Trauma21
-
46 Pediatric ENT Anatomy and Embryology With Radiology Correlates36
-
47 Acute Pediatric Airway28
-
48 Chronic Pediatric Airway Disease30
-
49 Pediatric Adenotonsillar Disease, Sleep Disordered Breathing and OSA41
-
50 Congenital Malformations of the Head & Neck22
-
51 Cleft Lip or Palate38
-
52 Pediatric Hearing Loss20
-
53 Microtia & Otoplasty24
-
54 Vascular Malformations16
-
55 Pediatric Head & Neck Tumors21
-
56 Anatomy & Embryology with Radiologic Correlates20
-
57 Principles of Wound Healing23
-
58 Facial Analysis23
-
59 Rhinoplasty & Nasal Reconstruction27
-
60 Periorbital surgery31
-
61 Lasers, Skin Resurfacing, & Alopecia28
-
62 Cosmetic Surgery for the Aging Neck & Face14
-
63 Botulinum Toxin & Fillers23
-
64 Facial Reanimation22
-
65 Skin Grafts & Local Flaps21
-
66 Regional & Free Flaps20
-
67 Principles of Trauma21
-
68 Facial Trauma54
-
69 Aerodigestive Anatomy & Embryology wuth Radiologic Correlates18
-
70 Laryngoscopy, Bronchoscopy, & Esophagoscopy32
-
71 Hoarseness & Dysphonia23
-
72 Voice Disorders & Voice Therapy20
-
73 Cough26
-
74 Dysphagia & Aspiration25
-
75 Benign Vocal Fold Lesions & Microsurgery29
-
76 Vocal Fold Paralysis17
-
77 Intubation & Tracheotomy26
-
78 Laryngeal Trauma17
