Assessment of Resp. Function in Clinical Patients Flashcards
(19 cards)
What is the most likely impact of hypoventilation on arterial blood gases in a patient breathing room air? Assume that gas exchange is normal.
Select one:
a. Both PaO2 and PaCO2 will increase
b. Both PaO2 and PaCO2 will decrease
c. PaO2 will increase and PaCO2 will decrease
d. PaO2 will decrease and PaCO2 will increase
e. PaO2 will be unchanged and PaCO2 will decrease
f. PaO2 will decrease and PaCO2 will be unchanged
PaO2 will decrease and PaCO2 will increase
If a patient hypoventilates alterations in arterial partial pressures of both oxygen and carbon dioxide are possible.
Reduced elimination of CO2 can lead to an increase in PaCO2 or hypercapnia.
Reduced delivery of O2 can lead to a decrease in PaO2 or hypoxaemia.
The question above stipulates that the patient is breathing room air, which has an oxygen content of approximately 21%, (or expressed as a fraction, FIO2 = 0.21). In patients breathing room air hypoventilation will cause alterations in both PaO2 and PaCO2, as described.
However anaesthetised veterinary patients generally breathe oxygen enriched gas and fractional inspired oxygen (FIO2) can approach 1 (or 100% O2). This additional oxygen helps maintain PaO2 at an acceptable level and will prevent hypoxaemia in the face of mild to moderate hypoventilation. In fact when breathing oxygen enriched gas hypoventilation must be severe to cause hypoxaemia. NB: this does not apply when breathing room air.
KEY POINT: Although alterations in both PaO2 and PaCO2 are possible as a consequence of hypoventilation measurement of PaCO2 is the preferred method to assess the adequacy of ventilation.
It is relatively easy to envisage how pathological thickening of the alveolar membrane might impede diffusion of gases and impair gas exchange. Understanding the impact of mismatched ventilation and perfusion is more difficult!
Matching of pulmonary ventilation and perfusion can be described by the ventilation/perfusion ratio (V/Q).
Consider an “ideal” area of lung where alveoli are both well ventilated and well perfused. This area of lung will have a V/Q ≈ 1.
A range of different V/Q ratios will exist at different levels in the lung.
Lung that is poorly ventilated but well perfused will have a V/Q ratio?
Lung that is well ventilated but poorly perfused will have a V/Q ratio?
- <1
- 1
If perfusion exceeds ventilation (V < Q) then the V/Q ratio will be less than 1. An extreme example of this type of V-Q mismatch is seen when an area of lung undergoes no ventilation but continues to be perfused. In this situation V/Q = 0.
If ventilation exceeds perfusion (V > Q) then the V/Q ratio will be greater than 1. An extreme example of this type of V-Q mismatch can occur if an area of lung is ventilated but not perfused (e.g. as a result of pulmonary thromboembolism). For this area of lung V/Q = ∞.
But what is the impact of V-Q inequality on arterial blood gases?
Consider an “ideal” area of lung that is both well ventilated and well perfused and has a V/Q ratio ≈ 1. Blood arriving at this area of lung, from the tissues, will be depleted of oxygen (PO2 ≈ 40 mmHg) and will contain an increased amount of CO2 (PCO2 ≈ 45 mmHg). Following gas exchange the blood draining this area of lung will have a higher PO2 (≈ 100 mmHg) and a lower PCO2 (≈ 40 mmHg). Don’t worry too much about the figures here, they are only included for illustration!
Now consider the PO2 and PCO2 of blood draining areas of V-Q mismatch: areas of poorly ventilated lung with a V/Q ratio less than 1 and areas of poorly perfused lung with a V/Q ratio greater than 1. How will blood gases differ from the “ideal” situation described above?
- Blood from lung units with a V/Q < 1 will have a PCO2 that is …
- Blood from lung units with a V/Q > 1 will have a PCO2 that is …
- Blood from lung units with a V/Q < 1 will have a PO2 that is …
- Blood from lung units with a V/Q > 1 will have a PO2 that is …
- higher than the “ideal” value
- lower than the “ideal” value
- lower than the “ideal” value
- higher than the “ideal” value
As a generalisation blood from areas with a V/Q ratio < 1 (i.e. areas that are poorly ventilated but well perfused) will have a relatively low PO2 and a relatively high PCO2. In effect, partial pressures of oxygen and carbon dioxide move away from those in an “ideal” well-matched lung unit (PO2 ≈ 100 mmHg and PCO2 ≈ 40 mmHg) and move towards those of mixed venous blood (PO2 ≈ 40 mmHg and PCO2 ≈ 45 mmHg).
In contrast, blood from areas with a V/Q ratio > 1 (i.e. areas that are well ventilated but poorly perfused) will have a relatively high PO2 and a relatively low PCO2. In this situation partial pressures of oxygen and carbon dioxide move towards those of inspired air (PO2 ≈ 150 mmHg and PCO2 ≈ 0 mmHg, for room air).
So what happens when blood from different lung units with different V/Q ratios mixes? What is the overall effect on PaO2 and PaCO2?
What is the likely impact of impaired gas exchange on arterial blood gases in a patient breathing room air? Assume that ventilatory function is normal.
Select one:
a. Both PaO2 and PaCO2 will increase
b. Both PaO2 and PaCO2 will be unchanged
c. PaO2 will increase and PaCO2 will decrease
d. PaO2 will decrease and PaCO2 will increase
e. PaO2 is unchanged and PaCO2 will decrease
f. PaO2 will decrease and PaCO2 will be unchanged
PaO2 will decrease and PaCO2 will be unchanged
Let us first consider the effect of impaired gas exchange on PaO2. Can areas of high V/Q ratio and increased PO2 compensate for areas of low V/Q ratio and decreased PO2? The simple answer is no, they cannot. The majority of blood oxygen content is present bound to haemoglobin and because the oxygen dissociation curve is non-linear an area of high V/Q ratio adds relatively little oxygen content compared to the decrease arising from an area of low V/Q ratio. Thus overall, inefficient gas exchange will decrease PaO2.
The effect of impaired gas exchange on PaCO2 is more variable. Providing ventilatory function is normal, any tendency for PaCO2 to rise will increase ventilatory drive and return PaCO2 to the normal range (NB: chemoreceptors are very sensitive to changes in PaCO2). This is possible because the carbon dioxide dissociation curve is linear so areas of high V/Q ratio can compensate for areas of low V/Q ratio. An additional consideration is that carbon dioxide diffuses much more readily than oxygen and so is less affected by diffusion impairment. Thus overall, it is possible for a patient with impaired gas exchange to have a normal PaCO2. However the degree of impairment must also be considered! If gas exchange is severely impaired and the patient is hypoxaemic, then respiratory control becomes oxygen-dependent and the resultant increase in ventilatory drive may actually decrease PaCO2.
So far we have considered hypoventilation and impaired gas exchange as separate processes. In some clinical cases, e.g. a cat with a ruptured diaphragm, there may be impaired gas exchange and concurrent hypoventilation. In this situation PaCO2 may rise.
KEY POINT: Changes in both PaO2 and PaCO2 are possible but oxygenation (e.g. PaO2) provides the best indicator of the efficiency of gas exchange.
what are the disadvantages of measuring arterial blood gas analysis
- invasive (an aerterial blood sample is required)
- It provides information about a specific time-point rather than continuous data
- Blood gas analysers can be expensive to purchase and run
- Samples must be collected and handled correctly to prevent artifacts (e.g. no air bubbles!)
what is a non-invasive alternative to arterial blood gas analysis
capnography
the partial pressure of carbon dioxide (PCO2) in respired gases is measured continuously as the patient breathes in and out. Respired gases are typically withdrawn from the breathing apparatus and analysed at the level of the monitor (known as sidestream capnography).
At which time-point (A, B, C, D etc) does inhalation start?

Inhalation begins at time-point D and PCO2 immediately starts to fall. Inspired gas does not normally contain CO2 and so the inspiratory baseline (between time-points E and A) should be at zero.
D
At which time-point (A, B, C, D etc) does exhalation start?

Exhaled gas will contain CO2 and so on first glance we might expect that time-point B, when PCO2 first starts to rise, might mark the start of exhalation. In fact exhalation starts at time-point A.
NB: the initial gas exhaled will have occupied non-respiratory parts of the upper airway, such as trachea and bronchi. It is known as deadspace gas. It will not have participated in gas exchange and therefore will not contain CO2.
A
Gas exhaled between time-points A and B is composed of …
Gas exhaled between time-points B and C is composed of …
Gas exhaled between time-points C and D is composed of …

- mostly deadspace gas from the upper airway
- mixture of alveolar and deadspace gas
- mostly alveolar gas
Exhalation starts at time-point A. The initial gas exhaled, between time-points A and B, will comprise mostly deadspace gas from the non-respiratory parts of the airway. Between time-points B and C, a mixture of deadspace gas and alveolar gas will be exhaled. The phase of the capnogram between time-points C and D is called the expiratory plateau and gas exhaled at this point is mostly alveolar in origin.
Gas exhaled at the very end of expiration (just before time-point D) will comprise only alveolar gas, which has undergone gas exchange. This gas will have equilibrated with pulmonary capillary blood and so will have a PCO2 that is very close to the PaCO2. The PCO2 of this “end of breath” sample is termed end tidal CO2 (or ETCO2). It is displayed on capnometers and capnographs and provides a non-invasive approximation of PaCO2. The normal value for ETCO2 in the dog is 4.6 - 6 kPa.
what is the amount of oxygen dissolved in arterial plasma expressed as
PaO2
how can the amount of oxygen bound to hemoglobin be determined by
pulse oximetry
What information do pulse oximeters typically provide?
Select one or more:
a. Haemoglobin concentration
b. Saturation of arterial haemoglobin with O2
c. Signal quality
d. Arterial partial pressure of O2
e. Respiratory rate
f. Pulse rate
Saturation of arterial haemoglobin with O2, Pulse rate, Signal quality
Saturation of arterial haemoglobin with O2 (SpO2) and pulse rate are displayed numerically
In addition most pulse oximeters include some form of signal quality indicator. In order to assess the saturation of arterial haemoglobin the pulse oximeter must differentiate between arterial and venous haemoglobin. This is achieved by selecting the pulsatile component of the signal, which can be attributed to arterial blood flow. If the overall signal quality is poor then arterial and venous components of the signal cannot be readily distinguished and errors in SPO2 measurement are likely. You could say that the signal quality indicator tells us whether we can trust the SpO2 reading displayed!
On the pulse oximeter shown the signal quality indicator is simply the colour of the flashing light, circled in green. If the light flashes green then the signal quality is acceptable, whereas a red/orange flashing light indicates poor signal quality.
Alternatively some pulse oximeters display a plethysmographic waveform that represents the cyclical changes in tissue volume related to inflow of arterial blood. The presence of a well-defined waveform implies good signal quality. Compare the 2 plethysmographs below: the first trace is normal but the second suggests poor signal quality
The relationship between PaO2 and SpO2 is described by a sigmoid curve, the haemoglobin dissociation curve (or oxygen dissociation curve).
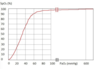
Note how steep the curve is between 0 and 60 mmHg. Within this section of the curve a small change in PaO2 results in a large change in SpO2. In contrast the upper portion of the curve, between 60 and 600, is very flat and at this level a large change in PaO2 results in very little change in SpO2.
Using the haemoglobin dissociation curve shown, can you relate PaO2 to SpO2 in the following scenarios?
- A healthy anaesthetised dog, breathing 100% oxygen, has a PaO2 over 500 mmHg. What % SpO2 would you expect?
- A healthy dog, breathing room air, has a PaO2 of 100 mmHg. What % SpO2 would you expect?
- A patient is considered hypoxaemic if SpO2 is < 90%. What is the corresponding PaO2, in mmHg, below which a patient is considered hypoxaemic?
- What PaO2, in mmHg, corresponds to an SpO2 of 65%?
- 95
- 95
- 60
- 40
In a healthy dog with a PaO2 of 100 mmHg the saturation of haemoglobin with oxygen will be close to 100% (certainly > 95%). Increasing PaO2 to over 500 mmHg by increasing the fractional inspired oxygen will result in little further increase in SpO2 because of the shape of the dissociation curve (i.e. its flat top).
Hypoxaemia can be defined as an SpO2 of less that 90% or a PaO2 of less than 60 mmHg.
Using the dissociation curve, an SpO2 of 65% will correspond to a PaO2 of 40 mmHg. However this is a slightly contrived question! Most pulse oximeters in clinical use do not provide accurate readings once SpO2 falls below about 75%.
You have anaesthetised a healthy dog for a routine ovariohysterectomy. You are worried about the patient’s breathing so you look at the capnograph which is connected to the patient.
Based on this monitor screen fill in the following gaps.
The respiratory rate is ____ breaths per minute
and the end tidal CO2 is ____ kPa.

- 8.8
- 5/min
in this case the end tidal CO2 is
and this results in too

- too high
- respiratory acidosis
The normal range for end tidal CO2 is 4.6-6 KPa in dogs. You may see this reference range quoted in mmHg too (35-45 mmHg) but these are not the SI unit.
Therefore this patient’s ETCO2 is too high. We have hypercapnia
End tidal CO2 is a surrogate measure of the arterial partial pressure of carbon dioxide (PaCO2) and the two are essentially the same in most cases. To measure the PaCO2 we would have to take an arterial blood gas sample which is not only technically challenging and doesn’t give us a continuous measure (we only get the value at the moment we took the sample). This is why capnography is such a useful monitor as it is non invasive but gives useful and real time information.
As the PaCO2 is high, this will result in a respiratory acidosis which if unopposed will reduce the pH of the blood. This is because dissolved CO2 reacts with water to produce carbonic acid (according to the Henderson-Hasselbalch equation).
Based on what you have concluded about the information from the capnograph above the dog is ______
what is the most likely cause
and what is the most appropriate solution
- hypoventilating
- anaesthesia induced resp. depression
- start ventilating the dog to reduce the ETCO2
The dog is hypoventilating as the CO2 has risen. Remember that the arterial CO2 partial pressure is inversely proportional to the alveolar ventilation (i.e. how much air is moved in and out of the alveoli per minute).
Common anaesthetic drugs such as the inhalant agents and the opioids cause hypoventilation via a central mechanism (depression of the respiratory center) and this is very commonly seen under anaesthesia. There are many other causes of hypoventilation and it may arise as a result of pathology at multiple different points along the respiratory control pathway. The following list is far from exhaustive and it is not necessary to learn individual conditions here!
Central depression e.g. anaesthetics as seen here but also certain neurological diseases
Neuromuscular diseases affecting the nerves and muscles which control respiration e.g myaesthenia gravis, tetanus and botulism
Respiratory diseases e.g. airway obstruction, severe lung disease and thoracic conditions which restrict the movement of the lungs
Animals may also hypoventilate to generate a respiratory acidosis in order to compensate for a metabolic alkalosis but the magnitude of this is small (if present at all) and wouldn’t explain the high CO2 seen here.
Too much oxygen will not reduce respiratory drive as oxygen partial pressure doesn’t control respiration unless it becomes very low (<60mmHg or 8 KPa) where it stimulates respiration causing hyperventilation. Therefore 100% oxygen as provided under anaesthesia won’t be the cause of the hypoventilation.
The simplest way to reduce the ETCO2 here would be to commence ventilation of the animal to increase the alveolar ventilation. In practice we might also try to reduce the concentration of anaesthetic we were using before doing this as respiratory depression from anaesthesia is dose dependent. Therefore by using less anaesthetic we should get less respiratory depression provided we use enough to keep our patient asleep!
Based on this monitor screen fill in the following gaps.
The respiratory rate is ____ breaths per minute and the end tidal CO2 is ____ kPa.

- 51/min
- 3.2
in this case the end tidal CO2 is _____ and this results in _____

The normal range for end tidal CO2 is 4.6-6 KPa in dogs.
Therefore this patient’s ETCO2 is too low. We have hypocapnia
As the PaCO2 is low, this will result in a respiratory alkalosis which if unopposed will increase the pH of the blood. This is because dissolved CO2 reacts with water to produce carbonic acid (according to the Henderson-Hasselbalch equation). If there is less CO2 there will be less acid and the pH of the blood will become more alkaline compared to normal.
The correct answer is: In this case the end tidal CO2 is [too low] and this results in [a respiratory alkalosis].
Based on what you have concluded about the information from the capnograph above the dog is ________
what is the most likely cause _______
And what is the most appropriate solution _______

- hyperventilating
- anaesthesia becoming too light
- increase concentration of the anaesthetic derived
There are a number of possible causes of hyperventilation.
Hyperventilation can occur in situations that cause pain, fear or distress and this is also true in anaesthetised animals. Hyperventilation can be associated with inadequate anaesthetic depth and can also occur as a response to noxious stimulus (especially if the patient is also too “light”). Because of the timing of the capnograph change in this case, “light” anaesthesia is the most likely explanation and the depth of anaesthesia should be increased.
Hyperventilation can occur secondary to hypoxaemia. If there is a failure of gas exchange leading to hypoxaemia or a failure of oxygen delivery to the patient (e.g. anaesthetic machine fault) then the animal will hyperventilate in an attempt to compensate. While this is certainly a possibility in this case, the timing of the change (during application of towel clips) makes the above option more likely.
Hyperventilation can also occur as a compensatory response to a metabolic acidosis as hyperventilation will cause an opposing alkalosis. However this is unlikely in this case due to both the magnitude and the timing of the change.
