Case 06 Flashcards
(10 cards)

called to review septic ac joint tap
HPI
atraumatic shoulder pain–ED-NSAIDS/Sling
Ortho- Cortisone SAS
Ortho- Ordered MRI after 4 weeks of treatment
PMH- gastric sleeve, electrician, RHD
Constitutional
BMI-36
RUE-
TTP, mass/warm
limited ROM/ no pain with
ADD/ER
Labs-13.2/5.3/40
127k cells/GS+/Culture–MSSA

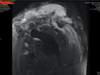
Pyomyositis with abcess in deltoid
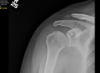
Septic AC joint
DC osteomyelitis
GH joint preserved
Labs/ESR/CRP/WBC
Cell count/GS/Culture

- Ordered labs to evaluate for infection vs tumor vs exudate
- Emergent vs Urgent intervention
- obtained curbside surgical consults and reviewed the literature
- organize team and develop surgical plan
- Medical clearance/ID and pathology involvement

Surgical Decision Making–
- GH Intra-articular?
- SAD- (scout team eval)
- DCE
A. how much?
B. open vs arthoscopic
Iatrogenic CC joint instability
- Other pathology found

- assess GH joint-dont contaminant- minimally invasive
- SAS–LOA/debridement/ scout team–arthroscopic access the best route to full debride with low morbidity
- Open DCE
remove bone with osteo
debride and Irrigate deltoid abscess.
- Other biceps tenotomy


DCE technique recommends 8-10mm removal but this was in the setting of osteomyelitis
Care to avoid CC ligaments (conoid) and cause Iatrogenic CC instability
Need to remove infected bone
specimen for path

admitted to hospital for 4 days of IV antbiotics
Given PICC line and discharged home
6 weeks in a sling with office follow-up
COVID restrictions
1 year follow-up


1 year follow-up
asymptomatic
back to work
CC instability or bad x-ray?