Case2 Flashcards
(6 cards)

Patient is a 19-year-old man who sustained an isolated left mid-shaft clavicle fracture after a fall while skateboarding. Patient has significant past medical history for non-smoker, right-hand-dominant, active and generally in good medical condition.

Relevant physical exam findings were most notable for mild skin tenting of the left shoulder, tenderness at the fracture site, uncomfortable in a sling, distally neurovascular intact in left upper extremity.
Interpretation of laboratory and imaging studies with notes most notable for left midshaft clavicle fracture with greater than 100% displacement and 2 cm shortening.
Pre-op labs were normal including COVID.

I had a long discussion with the patient regarding surgical and nonsurgical options. It is clear that patient was in severe pain and that the best indication for him was pain control to undergo surgery. We did also talk about the controversies in fixing this fracture type and that how some people will have better long-term outcomes with surgery as opposed to certain nonsurgical options. Nonsurgical option would be sling for approximately 6 weeks and pain control.

Once in the operating room the patient was placed in the beachchair position with intraoperative fluoroscopy used to confirm fracture site as well as assist in plate and screw placement as well as reduction confirmation. Anesthesia placed an interscalene block with local lidocaine and Marcaine placed by me.
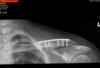
My surgical approach was directly over the clavicle including skin soft tissue skin flaps intact dissecting down through the platysma.. I was able to control fracture fragments and when I evaluated the fracture I identified comminution at the fracture so I did not place a lag screw. The fracture fragment did allow for compression using the plate. I used a superior plate location , 7 hole, titanium with some contouring. I placed on screw within the distal bone, followed by an eccentric screw on the other side of the fracture (away from the fracture)to compress the fracture. I then placed 3 3.5mm cortical screws bi cortically on each side which is excellent purchase into the bone for plate stabilization. I confirm fracture reduction and instrumentation fluoroscopically at the end of the case. Surgical time was approximately 1 hour with blood loss of 25cc estimated. Patient had very good bone and head I had excellent purchase using cortical screws x 6; I did not feel there was any need for additional locking screws for stabilization. I was concerned one screw was close to the fracture site I was able to get excellent purchase I did not feel I needed to fortify that with a locking screw. Wounds were closed in layers with monocryl subcutical closure

Patient was discharged to home with postop instructions to remain in sling for 4 to 6 weeks and to be non weight bearing the operative upper extremity. Per standard postoperative protocol patient was given Multimodal pain medications.
The patient did not attend his initial postoperative visit but I was able to see him at 6 weeks after surgery was able to assess his function and the images. His recovery at that point was routine and as expected. He was instructed to follow-up in 3 months for maximal medical improvement assessment confirmation of radiographic healing however the patient declined secondary to Covid concerns.
