Pulmonary Portion Flashcards
(118 cards)
what are the three broad types of pneumonia source categories? which one is most common? which are most difficult to treat?
- community acquired pnuemonia (CAP)
**most common**
- healthcare/hospital acquired pneumonia (HCAP)
- most difficult to treat - ventilatror associated pneumonia (VAP)
what are four important ways to reduce ventalator associated pneumonia (VAP)?
- avoid ET tube
- keep head of bed elevated
- reduce sedation
- hand washing
what is important to do once you have finished treating pneumonia?
post treatment xray
want to make sure everything is cleared up and that the treatment has worked!
what is the most common organism seen in pneumoniae overall?
s. pneumoniae
what four patient populations make you at an increased risk for pneumonia?
- ETOH
- asthma
- immunosupressed
- elderly
Typical pneumonia
what are four common organisms associated with this and their characterist sputum color? how long do symptoms increase? what are some of the things on the long list of symptoms
“common symptoms”, usually responsive to B-lactams
#1 most common: streptococcus pneumoniae (rusty red color)
#2: haemophilis influenzae (green sputum)
staph aureus
klebsiella (currant jelly)
pseudomonas (foul smelling)
SX:
1-10 day increase in cough, purlulent sputum, SOB, dullness to precussion, rigors, tachycardia bronchial breath sounds, tactile fremitis (say 99), friction rub, pleuritic chest pain, night sweats
atypical pneumonia
“walking pneumonia”
usually unresponsive to beta lactam, use macrolide or fluorquinolone
1. mycobacteria pneumoniae (bullous myringitis..ear)
2. chlamydia pneumonia
3. legionella
4. viruses->
(RSV and parainfluenze in kids, and influenza in adults)
PE: often normal physical exam, can have extrapulmonary symptoms
DX: use macrolides (erythromycin, azithromycin, clarithromycin, doxycycline) or fluoroquinolones
what are the three most common organisms that cause community acquired pneumonia (CAP)?
#1: streptococcus pneumoniae
#2: haemophilis influenzae (esp in COPD)
#3 mycoplasma pneumoniae (atypical)
what are the three common organisms that cause hospital acquired pneumonia?
- gram negative pseudomonas
- ancinetobacter
- staph aureus
what is the mortality rate in hospital acquired pneumonia?
50-70%
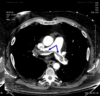
what are the five tests you use to diagnose pneumonia?
- clinical syndrome, empirically
- gram stain- GCP
- sputum culture
- urine tests (only in legionella and pneumococcus)
- xray showing white infiltrate
streptococcus pneumoniae=
pneumococcus
they are the same thing, so if used in a test question, they mean the same thing, its just an abreviated name for this **important since this is the most common organism to cause pneumoniae**
if a patient has pneumonia with MRSA, what should you use to treat?
vancomycin
streptococcus pneumoniae in pneumonia
(what color is the sputum? what is it sensitive to? what can happen if this is systemic? is there a immunization for this?)
- rusty blood colored sputum
- beta lactam sensitivity
- if systemic can cause confusion
**immunizable** this is what the vaccine is for!
what is the treatment for patients with pneumonia? how long is the treatment regimen?
- 80% can be treated as outpatient with macrolide azithromycin/erythromycin/clarithromycin
(atypical or “walking pneumonia)
- if ths same patient has chronic illness combine with beta lactam
- if MRSA infection use vacomycin or fluroquinolone
**5- 14 day treatment**
Explain the new vaccine regimen that is reccomeded?
PVC13: childhood vaccination
PV23: used in 65 +
****new recommendations say 65+ recieve BOTH, adults get PCV13 first then PV23 second 8 weeks later***
if they have already had PV23, wait a year and give PVC13
explain which pneumonia organism these populations are at the most risk to get:
ETOH-
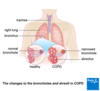
COPD-
CF-
Air-conditioning-
children
Children
ETOH- klebsiella
COPD- haemophilis influenzae
CF-pseudomonas
Air-conditioning-legionella
children
Children
what is the most common lung cancer seen in non smokers?
adenovirus
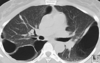
general bronchogenic carcinoma
“Lung cancer”
what is this the leading cause of? what are the two types? where are the four locations these mets are likely to spread? what is the main cause of these? what are 7 symptoms associated with lung cancer in general?
leading cause of cancer in men and women
made of two categories:
- small cell lung carcinoma
- non small cell lung carcinoma
mets to brain, bone, liver, lymph
SX:
****ASYMPTOMATIC, mostly incidental finding on CXR****
- ***change in nature of cough (squamous, small cell)
- hemoptosis
- vague nonpleuritic chest pain
- reccurent pneumonia
- WEIGHT LOSS ANOREXIA ASTHENIC (CLASSIC)
- HYPERCALCEMIA, don’t miss this
cigarette smoking is the main cause, 85% of lung cancer in smokers

small-cell carcinoma “oat cell”

is this fast or slow? WHERE IS IT LOCATED? what is the doubling time? what are the 6 paraneoplastic syndroms associated with it? what is the treatment? what is the difference between limited and extensive stage?
bad actor!!-grows quickyl metastasizes early!! assume m micrometasizes on presentation!
CENTRAL bronchial epithelium (near hilum because thats where all the vessels are so it can get a lot of nuitrients)
doubleing time: 30 day!!!
limited stage: tumor on the same side of chest, supraclavicular lymph nodes, or both (20% 2 year survival)
extensive stage: anyhting beyond limited stage (5% 2 year survival)
associated paraneoplastic syndromes: cushings, hyponaturemia, SAIDH, periphreal neuropathy, eaton lambert, cerebral degeneration
TX: since it matastasizes so quickly, CHEMO is the treatment
squamous cell cancer

which cells does this occur in? where is it located? how can you dianose/what is major symtom? what is a random paraneoplastic syndrome associated with this? what is interesting about the metastsis of this? who is this most common in?
MOST COMMON NON-SMALL CELL IN SMOKERS!!!
basal cells of bronchial epithelium
centrally located, frequency hemoptysis and change of cough, CAVITATION
hemoptosis diagnosed with cytology
late metastasis–so if you catch it early in the patient the prognosis is better!
paraneoplastic synderome: hypercalcemia
TX: surgical

adenocarcinoma

what is this the most common of? where does the cancer occur and where does it appear? what does it metastasize to? what is the treatment? what are two paraneoplastic syndromes? what can you get it from? smokers or nonsmokers?
most common bronchogenic CA
common in non-smokers
peripheral, lung parenchyma
originates in the mucous glands of tracheobrachial tree and appears in the periphreay of lung
moderate growth and metastatic rate
NON SMOKERS, can get from ASBESTOS!!!
paraneoplastic syndrome: thrombophlebitis, PTH-rp
TX: surgical

large cell cancer
where is this located? what is the doubling time? is there metastasis? what is the paraneoplastic syndrome? what is the treatment?
periphreal or centrally located
cavitation
rapid growth
early metastasis
doubling time 100 days
paraneoplastic syndrome: gynecomastic
TX: surgical

bronchial carcinoid tumor
what type of tumor is this? where else is it commonly found? describe what this tumor would look like if you saw it? what does it secrete (4), what are two symptoms you can have with this? what is the treatment?
CENTRAL neuroendocrine tumor, slow growth, slow mets
also commonly found in GI tract
typical: SESSILE (attached to base) or pedunulated (cylander)
atypical
pink/purple well vascularized central tumor, pedunculated or sessile
secretes SEROTONIN, ACTH, ADH, MSH
often asymptomatic, but can have hemoptosis and c_arcinoid syndrome_ (diareah from increased serotonin and left sided hear fibrosis)
TX: steroids and surgery, resistant to chemo and radiation