GI Portion Flashcards
(145 cards)
gastroesophageal reflux disease
what is this?
population common in?
percent in US?
5 complications it can lead to
most common dxs of esophagous 15-20% US, common in pregnancy

transient relaxation of lower esophageal spincter LES leading to gastric acid reflux that causees damange to esophagus and spincter and can lead to:
1. esphagitits- 50% will get this!!!
2. esophageal stricutre
3. barrettes esophagous
4. esophageal adenocarcinoma
- hiatial hernia
-
GERD
what are 6 sxs?
1 thing to keep in mind about sxs?
- heartburn, restrosternal and postprandial
substernal pain/discomfort most commong 30-60 minutes after a meal
worsens when laying down or recumbant
- regurgitation (vomit burp)
spontaneous reflux of sour bitter gastric contents in mouth
- dysphagia (discomfort)
cough at night from acid asipiraiton
- reccurent pneumonia
- sxs temp relieved with antacids
- can radiate to arm/jaw
***keep in mind sxs don’t correlate with dxs progression so can’t tell how much damage has been done**
what is the pathway for txing GERD?
6
- lifestyle adjustments
- OTC antacids-2 weeks
- H2 receptor antagonists
- Proton pump inhibitors
**if these fail EDG**
- prokinetics
- surgical

GERD
3 dx options
6 reasons of when it is not appopropriate to use the first line dx
- empirically first line unless (below)
- esphagogastroduodenoscopy(EGD) if high risk or tx has failed
a. over 50
b. weight loss
c. melena
d. odynophagia pain with eating
e. heavy alcohol or tabacco
f. non repsonsive to tx - modified/full barium swallow
what are the lifestyle changes a patient should make to relieve sxs of GERD?
5
- avoid eating 2-3 hours before bed
2. elevate head of bed
3. loose weight
- avoid acidic food, chocolate, peppermint, ETOH, coffee
- stop smoking
why is it important to treat GERD?
prevent cancer aka barrette esophagus because the damange from acid makes this more likely to occur
what is the emergency cocktail you give someone in the ED for heart burn?
- benadryl
- lidocaine
- maalox
what is the most common cause of esophagitits?
GERD, 50% of patients with GERD have esophagitits
esophagitits
what is this?
5 general causes?
4 sxs
inflammation of the esophagus, esp in immunocomprimised
- viral
- bacterial
- paraistic
- abx induced
- radiation or chest cancers
sxs;
- odyniaphagia
- dysphagia
- substernal chest pain
- oral thursh
esophagitis
herpes liabilis (HSV)
3 SXS?
2 DX?
1 TX
N/V/ chills
herpetic vesicles on nose/lips
dx:
1. endoscopy showing small vesicles or superficial lesions
2. culture esophageal lesions
TX:
ACYCLOVIR 7-21 DAYS!!!
ESOPHAGITIS
VARICELLA-ZOSTER
1 dx?
tx?
N/V fever chils
DX:
endoscopy: vesicles or confluent ulcers
Tx:
- usually resolve spontaneously but can cause necrotizing esophagitits
- ACYCLOVIR!!!!
esophagitis
CMV
who does this occur in?
characteristics of ulcer? 2
3 sxs?
1 tx?
only occurs in immunocomprimised patients
CREEPING ULCER or can be GIANT ULCER
sxs:
odyniaphagia
persistent CP
hematememis
Tx:
IV GANCICLOVIR
esophagitis
candidia
who does it occur in?
3 complications?
1 dx?
1 tx?
occurs in immunocomprimised host
can cause complications:
- bleeding
- perforation
- stricture
dx:
endoscopy: small yellowwhite raised plaques
tx:
oral or IV fluconazole!!
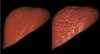
barrett’s esophagus

how does this occur? what hcanges?
what are they at increased risk for? how much?
metaplastic changes in which the stratified squamous** is replaced by the **columnar epithelium that is typically found in the duodenum….extens poximally from LES from repeated exposure to acid esp with GERD (thats why the cells change to this type because its the same exposure the duodenum gets)
increases risk for adenocarcinoma 5-10%
this change increases risk for neoplastic changes/cancer 40-100 times greater than general public
barettes esophagus

2 dx rules?
3 tx?
DX:
EDG every 2 years with bx to check for neoplastic changes
if there is high risk dysplasia, consider surgrical resection
TX:
**more txing symtpoms unless surgical intervention**
- antacids
- H2 blockers OTCs
- PPIs
esophageal cancer
what are the two types?
frequency?
prognisis?
who is more common?
types:
- adenocarcinoma
- squamous cell carcinoma
prognosis typicaly poor, 5 year survival 10-13%
both appeare with equal frequency
males more common than females
esophageal cancer:
adenocarcinoma
where do you find this?
4 most important RF?
2 protective

distal esophagus
RF:
- reflux over 20 years
- Barrettes esophagus-almost all cases
- obesisty
- caucasion males
- smoking increases risk (not main)
Protective effects:
- fiber
- NSAIDS (seems counterintuitive)
esophageal cancer:
squamous cell carcinoma
prevalence?
location?
4 RF?
key point to remember?
prevalence is decreasing
middle esophagus
RF:
- smoking
- alchohol
- diet low in fruits and veggies
- achalasia increases risk 16 x
*** accounts for 90% of all squamous carcinoma in US***
esophageal cancers
sxs
1 early
3 late
SXS:
early:
1. transient “sticking” of food that turns to PROGRESSIVE DYSPHAGIA
later:
- retrosternal pain/burning
2.iron deficient anemia -loss from chronic cancer, but not enough to notice hememensis or occult
3. tracheobronchial fistula
late complication where the esophageal wall infilates the stem bronchus causeing intractable coughing with frequent pneumonia
_***if this occurs person has less than four weeks to live***_
in esophageal cancer, when would you expect to see the weight loss and dysphagia?
when the lumen is less than 13 mm
esophageal cancer
2 DX
2 STAGE
dx:
- barium studies
- endoscopy
Staging:
- CT OF CHEST AND UPPER ABDOMENT
2. PET SCAN
where are adenocarcinomas and squamous cell esophageal cancers found?
adenocarcinoma: lower 1/3
squamous: middle esophagus
esophageal varices

what is this?
what causes this?
mortaltiy rate?
MOST COMMON CAUSE?
emergency!!!
dilation of the submucosal veins that develop in pts with portal HTN
patho: blood flow through the liver is diminished causing blood flow increase through the microscopic bood vessesl within the esophageal wall and the vessels dilate profoundly, and then continue to dilate until they are large enough to rupture
patient acutely ill, mortality rate 40-70%
MOST COMMON CAUSE OR PORTAL HTN IS CIRROSIS that causes this

where is the most common stie for esophageal varices? why?
distal esophagus at gastroesophageal junction because veins are most superficial here!!