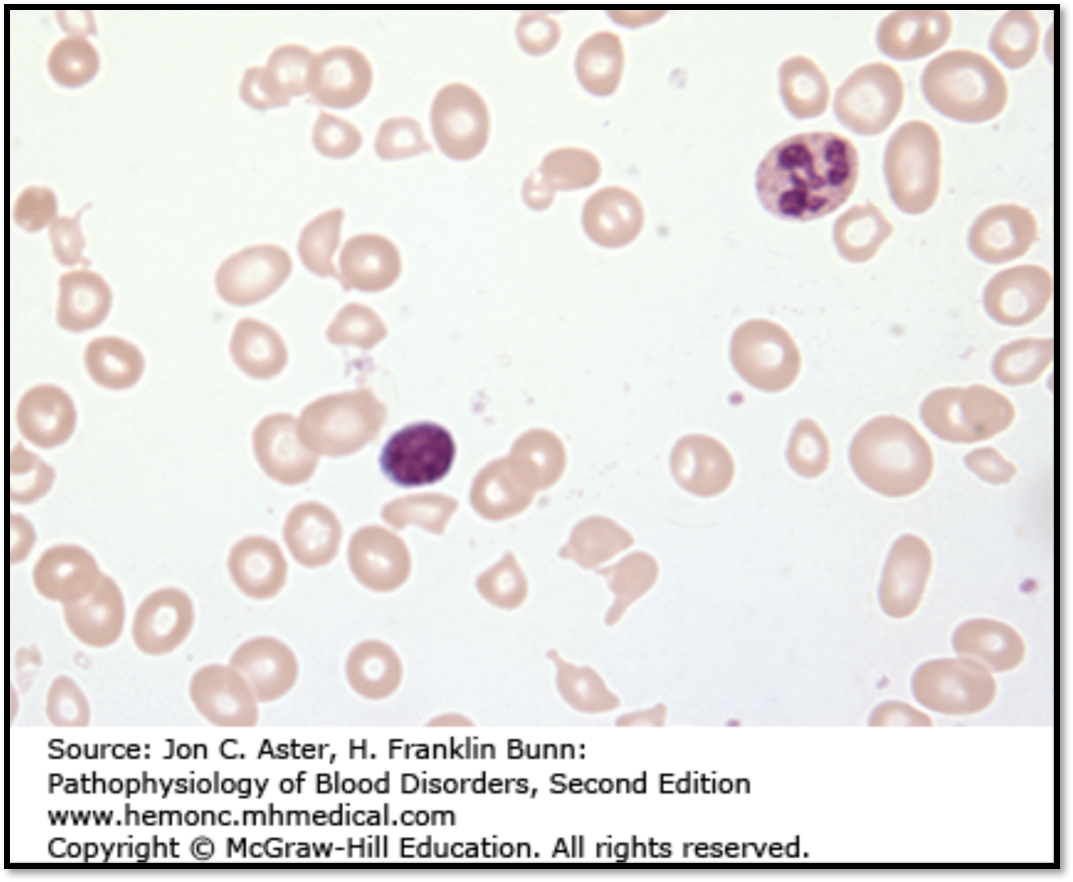
The attached image compares a marrow aspirate from a normal individual with the BM aspirate from an individual with the condition described below:
Vegetarian
Pallor, lemon yellow tinged skin
beefy red tongue
PS: hypersegmented neutrophils
What are the 3 key BM findings in this condition?
Deborah Dalmeida MD
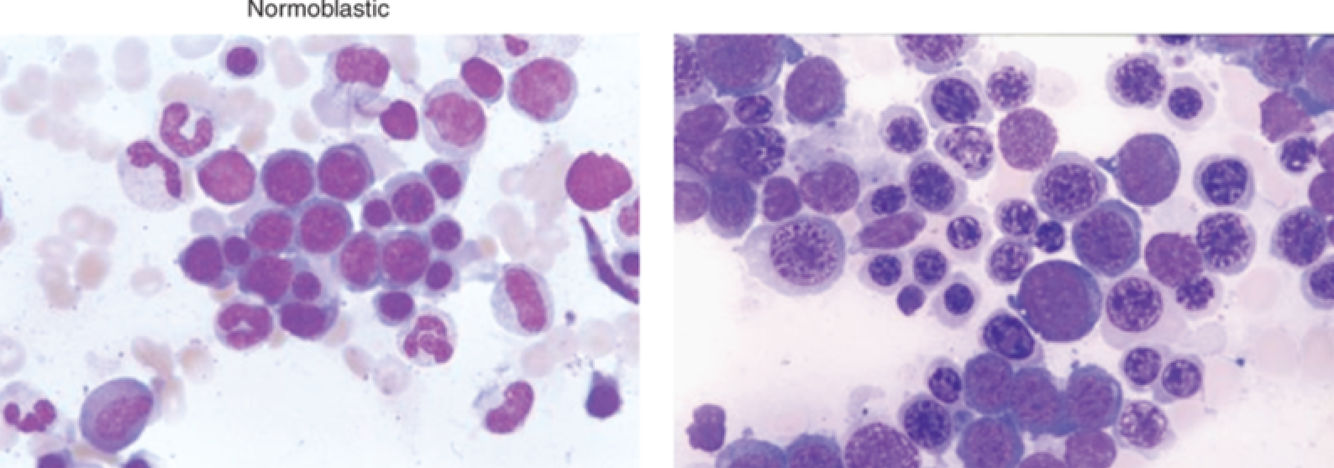
- Nuclear cytoplasmic dysynchrony - cytoplasmic differentiation, as assessed by increasing hemoglobin production, is normal, nuclear maturation is retarded
- markedly hypercellular
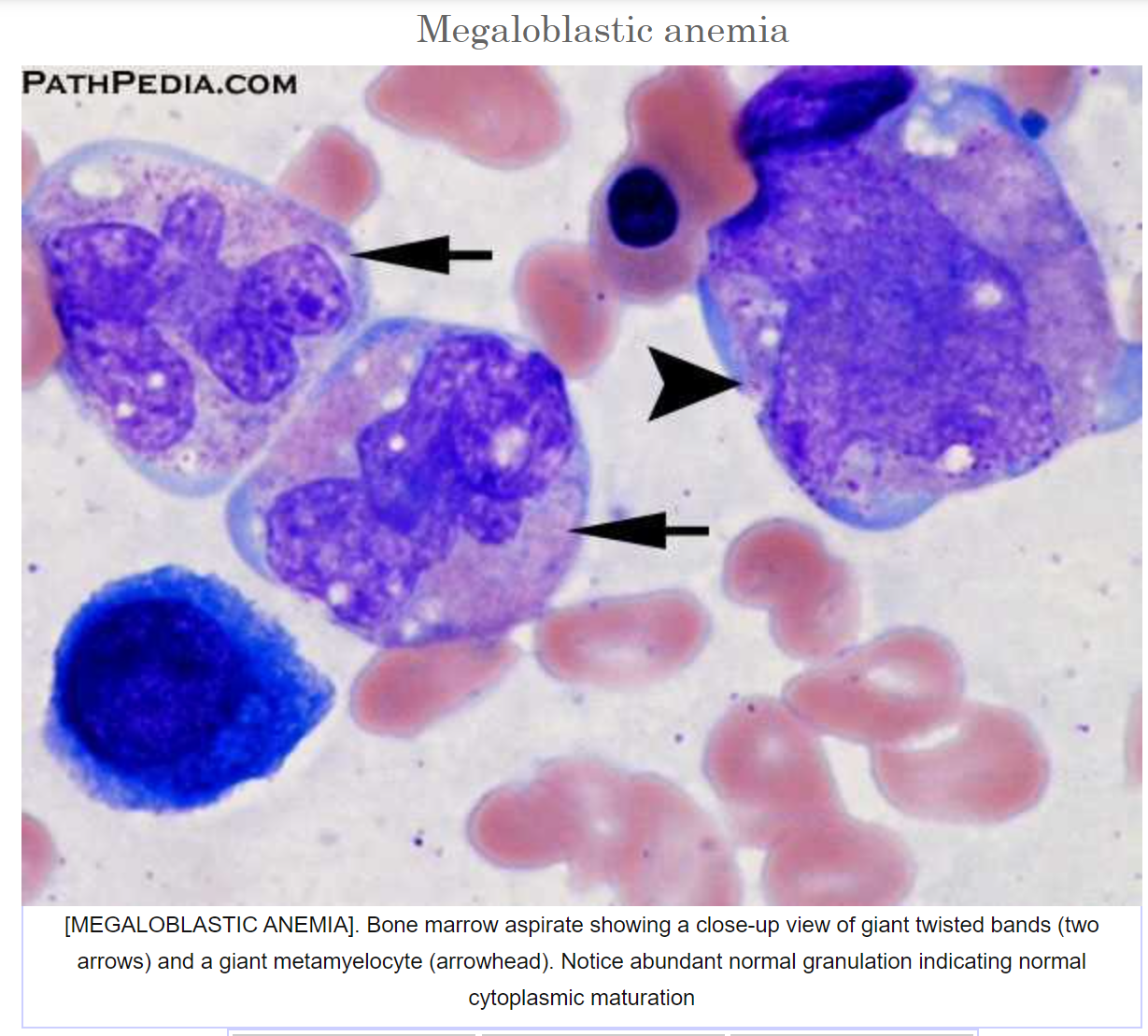
- giant metamyelocytes and band forms
Deborah Dalmeida MD
- 2 features of anemia of chronic renal failure on a peripheral smear
- Why do they develop anemia?
Deborah Dalmeida MD
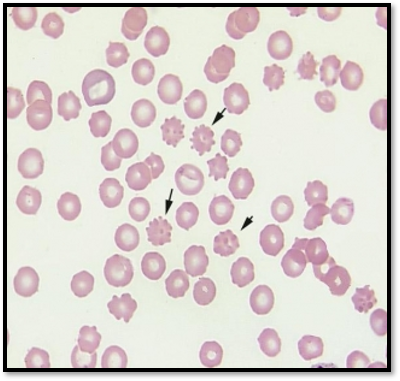
- normocytic anemia,presence of burr cells
- diminished synthesis of EPO
Deborah Dalmeida MD
peripheral pancytopenia (decreased RBCs, WBCs, platelets)
reticulocyte index <2
marrow hypoplasia
No splenomegaly
Deborah Dalmeida MD
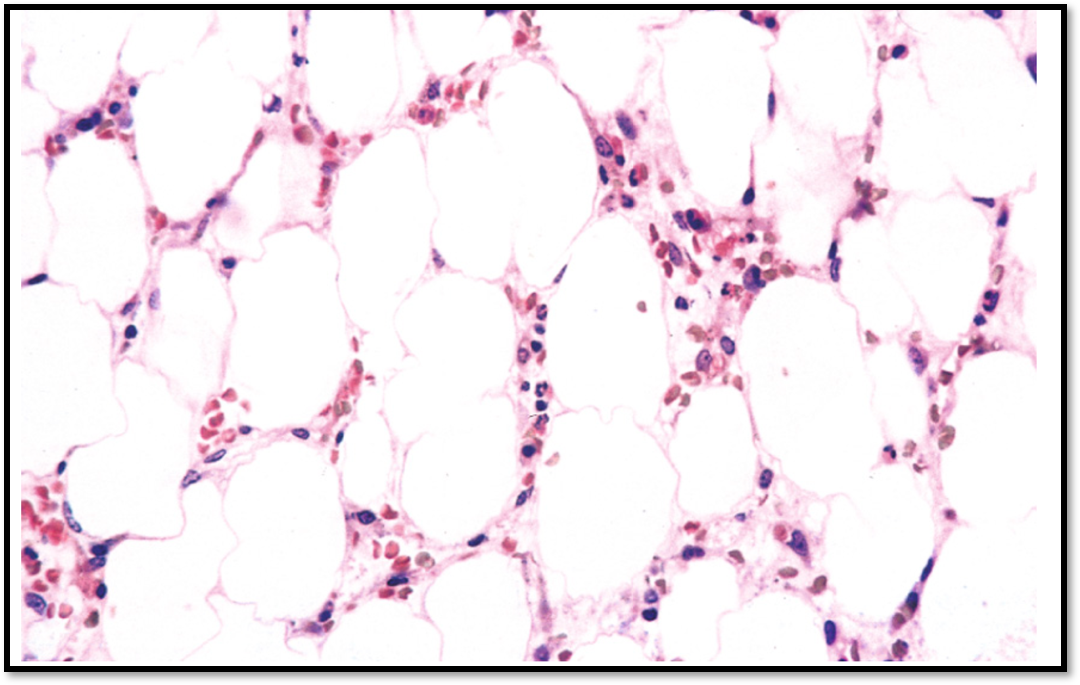
Aplastic anemia
Deborah Dalmeida MD
What features on a peripheral smear are characteristic of myelophthisic anemia?
Deborah Dalmeida MD
abnormal release of nucleated erythroid precursors and immature granulocytic forms ka leukoerythroblastic reaction
teardrop cells
Deborah Dalmeida MD
two important biochemical reactions requiring Vitamin B12
Deborah Dalmeida MD
- conversion of methylmalonyl-coenzyme A (CoA) to succinyl-CoA
- conversion of homocysteine to methionine.
Deborah Dalmeida MD
autoimmune disorder characterized by the destruction of gastric parietal cells
- What are the 2 types of antobodies produced?
- How does this disorder lead to megaloblastic anemia?
Deborah Dalmeida MD
- Antibodies against parietal cells and antibodies against intrinsic factor
- Parietal cells are the source of IF. Without intrinsic factor, food cobalamin cannot be absorbed in the distal ileum
Deborah Dalmeida MD
Time duration before a reticulocyte repsonse is observed in acute blood loss?
Deborah Dalmeida MD
5-7 days
Deborah Dalmeida MD
Differentiate folic acid versus Vit B 12 deificiency
Deborah Dalmeida MD
decreased folate levels in the serum or red cells.
serum homocysteine levels are increased, but methylmalonate concentrations are normal
neurologic changes do not occur.
Deborah Dalmeida MD
List 4 causes for Vitamin B12 deficiency apart from decreased intake.
Deborah Dalmeida MD
a. gastrectomy
b. ileal resection/disease
c. fish tapeworm infestation
d. bacterial overgrowth in blind loops and bowel diverticula
Deborah Dalmeida MD
How does methotrexate cause folic acid deficiency?
Deborah Dalmeida MD
Inhibits dihydrofolate reductase
Deborah Dalmeida MD
most common cause for folic acid deficiency
Deborah Dalmeida MD
alcoholism
Deborah Dalmeida MD
Lab findings in Vit B12 deficiency apart from PS and BM
Deborah Dalmeida MD
low serum vitamin B12 <200pg/ml
elevated serum levels of homocysteine
Elevated methyl malonic acid
MCV >110 fL
Deborah Dalmeida MD
Why do you get a slight increase in the level of nonconjugated bilirubin in the serum and a marked increase in serum lactate dehydrogenase (LDH) in megaloblastic anemia?
Deborah Dalmeida MD
increased rate of apoptosis of erythroid precursor cells due to derangement in DNA synthesis
Deborah Dalmeida MD
Stomach morphology in pernicious anemia
Deborah Dalmeida MD
Fundic gland atrophy
Intestinal metaplasia
Deborah Dalmeida MD
features of megaloblastic anemia on peripheral smear
Deborah Dalmeida MD
macro-ovalocytes
Anisocytosis
Poikilocytosis
Neutrophils are larger than normal and show nuclear hypersegmentation, having five or more nuclear lobules instead of the normal three to four
reticulocyte count is low
Deborah Dalmeida MD
- In whom does Parvovirus B19 infection trigger an aplastic crisis?
- How does it trigger an aplastic crisis?
Deborah Dalmeida MD
- In persons with moderate to severe hemolytic anemias, even a brief cessation of erythropoiesis results in rapid worsening of the anemia, producing an aplastic crisis.
- attaches to P antigen on the RBC membrane and destroys red cell progenitors
Deborah Dalmeida MD
Name the type of anemia described below:
space-occupying lesions replace normal marrow elements
Deborah Dalmeida MD
Myelophthisic anemia
Deborah Dalmeida MD
2 possible causes for myelophthisic anemia
Deborah Dalmeida MD
- metastatic cancer- breast, lung, and prostate
- granulomatous disease
Deborah Dalmeida MD
- 3 Signs of Subacute combined degeneration of the Spinal Cord
- What is the reason for demyelination?
Deborah Dalmeida MD
- posterior column (PC) - loss of vibratory sensation and proprioception (joint sense).
lateral corticospinal tract (LCST) - spasticity.
dorsal spinocerebellar tract (DSCT) - ataxia.
- lack of methyl-B12 for conversion of homocysteine to methionine. ↓SAM → ↓methyl group for Phosphatidylethanolamine conversion to Phosphatidylcholine for incorporation into myelin
Deborah Dalmeida MD
List 3 causes for pure red cell aplasia
Deborah Dalmeida MD
Parvovirus B19 infection
Diamond-Blackfan syndrome
Thymomas
Deborah Dalmeida MD
Identify this condition
a. normocytic normochromic anemia with reticulocytopenia
b. presents during the first 6 months of life
c. Short stature
Craniofacial – snub nose, wide spaced eyes
Thumb abnormalities – triphalangeal etc
Deborah Dalmeida MD
Diamond Blackfan Syndrome
Deborah Dalmeida MD
Which enzyme levels are elevated in Diamond Blackfan Syndrome?
Deborah Dalmeida MD
erythrocyte Adenosine deaminase
Deborah Dalmeida MD
-
HEMODYNAMIC DISEASE, THROMBOEMBOLIC DISORDERS AND SHOCK72
-
BLOOD VESSEL PATHOLOGY57
-
HEART PATHOLOGY -147
-
HEART PATHOLOGY -245
-
RENAL PATHOLOGY 158
-
RENAL PATHOLOGY 282
-
RENAL PATHOLOGY -346
-
RENAL PATHOLOGY 444
-
LOWER URINARY TRACT22
-
MUSCULOSKELETAL PATHOLOGY-129
-
MUSCULOSKELETAL PATHOLOGY-256
-
MUSCULOSKELETAL PATHOLOGY - 327
-
MUSCULOSKELETAL PATHOLOGY - 442
-
MUSCULOSKELETAL PATHOLOGY - 538
-
CELL INJURY, ADAPTATIONS AND DEATH - 142
-
CELL INJURY, ADAPTATIONS AND DEATH - 231
-
ACUTE & CHRONIC INFLAMMATION- 150
-
ACUTE & CHRONIC INFLAMMATION - 220
-
TISSUE REPAIR38
-
AMYLOIDOSIS28
-
NEOPLASIA-154
-
NEOPLASIA-233
-
ENVIRONMENTAL & NUTRITIONAL PATHOLOGY55
-
RBC DISORDERS-143
-
RBC DISORDERS-222
-
BLEEDING AND THROMBOTIC DISORDERS36
-
WBC DISORDERS - 146
-
WBC DISORDERS- 248
-
SKIN PATHOLOGY-145
-
SKIN PATHOLOGY-229
-
LUNG PATHOLOGY-145
-
LUNG PATHOLOGY -223
-
Female genital tract 157
-
BREAST PATHOLOGY28
-
MALE GENITAL TRACT56
-
KEY LAB VALUES30
-
Female genital tract 232
-
Disorders of pregnancy25
-
Diseases of infancy and childhood50
-
NUPY 1_Neurocytopathology, Congenital Malformations50
-
NUPY2_Eye Pathology39
-
NUPY 3_Movement disorders30
-
NUPY 4_Muscle weakness50
-
NUPY 5_Cerebrovascular disease58
-
NUPY6_Neurodegenerative Disorders20
-
NUPY7_Traumatic brain injury42
-
NUPY8_CNS &PNS tumors37
-
NUPY9_Pathology of CNS infections38
