DIT review - Cardiology 3 Flashcards
In the cardiac cycle graph, show were mitral and aortic valve opening and closing occur


What causes S1 and S2 heart sound
S1 = closing of mitral valve
S2 = closing of aortic valve
What causes S3 heart sound
- S3 = rapid flow of blood from the atria to the ventricles
- Occurs right after mitral valve opens
- Normal in children but not heard in adults
- Presence of S3 in adults indicates volume overload (e.g. congestive heart failure, advanced mitral or tricuspid regurgitation) or dilated ventricles
- Causes of S3 heart sound:
- Dilated cardiomyopathy, congestive heart failure, mitral regurgitation, L-to-R shunting
What causes S4 heart sound
- S4 = atrial contraction
- Not present in normal adults
- Caused by atrium contracting against a stiffened ventricle
- Causes of S4:
- Hypertrophic cardiomyopathy, aortic stenosis, chronic HTN with LV hypertrophy, post-MI
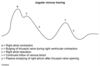
Label the jugular venous tracing graph

- A wave = atrial contraction
- C wave = ventricular contraction
- V wave = atrial filling against closed tricuspid valve
Describe what normal heart sound splitting is
- Inspiration = decreased intrathoracic pressure = increased venous return = increased RV filling = increased RV stroke volume = increased RV ejections time = delayed closure of pulmonic valve

Describe wide splitting
- Splitting occurs both in inspiration and expiration (but still more on inspiration)
- Due to conditions that delay RV emptying (e.g. Pulmonic stenosis, R bundle branch block)

Describe fixed splitting
- Occurs during right heart overload (e.g. atrial septal defect)
- ASD = L-to-R shunt = increased RA and RV volumes = increased flow through pulmonic valve such that, regardless of breath, pulmonic closure is delayed

Describe paradoxical splitting
- Due to conditions that delay aortic valve closure (e.g aortic stenosis, left bundle branch block)
- Normal order of valve closure is reversed so that P2 occurs before delayed A2
- On inspiration, P2 closes later and moves closer to A2, thereby “paradoxically” eliminated the split

What valves associate to what auscultation locations on the chest?

What murmurs are increased by inspiration?
- This decreases intrathoracic pressure, thus increased venous return to the heart
- Increased intensity of R heart sounds (e.g. Tricuspid murmur)
What murmur are increased by hand grip?
- This increases SVR, this increasing afterload
- Increased intensity of mitral regurgitation, aortic regurgitation, and VSD
What murmurs are increased by Valsalva maneuver?
- This increases intrathoracic pressure, thus decreasing preload (opposite of inspiration)
- Decreases the intensity of most murmurs EXCEPT increases intensity of hypertrophic cardiomyopathy
Holosystolic, high-pitched “blowing” murmur best heard at apex
Mitral regurgitation
Describe electrolytes responsible for each phase in cardiac myocyte fast action potential (Phase 4, 0, 1, 2, 3)
- Stage 4 (baseline negative state)
- Only “leaky” potassium channels open (K+ leaking out of cell - inward rectifier current)
- Stage 0
- Voltage gated Na+ channels open (after threshold -70 is reached by Na+ and Ca+ leaking through gap junctions)
- Na enters very quickly à fast depolarization
- Stage 1
- Initial repolarization – Na+ channels close and voltage gated K+ channels open (K+ leaves cell), causing repolarization
- Stage 2
- Plateau – Ca2+ channels open (Ca enters cells) – L-type channels
- Ca2+ and K+ channels pull voltage in opposite directions, so reach sort of plateau
- This is the phase that causes myocyte contraction (due to Ca2+ triggering more Ca2+ release from sarcoplasmic reticulum)
- Stage 3
- Rapid repolarization – Ca2+ channels close, so only K+ channels open
- But eventually the voltage gated K+ channels will close, leaving only open the “leaky” potassium channels, so there is membrane stabilization

Describe electrolytes responsible for each phase of pacemaker slow action potential (Phase 4, 0, 3)
- Stage 4
- Na+ channels (If – funny current) are open (Na+ enters cells) and allow depolarization (voltage gated K+ channels are closed)
- The rate of stage 4 depolarization is what sets the heart rate
- Stage 0
- Threshold reached where voltage gated Ca2+ channels open causing more rapid depolarization at threshold (-40)
- Ca2+ enters pretty quickly, but not as quickly as Na+ in stage 0 of myocytes à slow action potential
- Stage 3
- At threshold +10, voltage gated Ca2+ channels close and voltage gated K+ channels open (potassium leaves cell), causing repolarization (at -60, the voltage-gated K+ channels will close and Na+ channels will reopen)
- At certain threshold, K+ channels close, so Na+ is only channel open and cycle restarts
