Histopathology 10 - Upper GI disease Flashcards
(68 cards)
What is the “Z line” in the GI tract?
point at which epithelium transitions squamous → columnar

What are the 3 layers of the oesophageal wall?
Mucosa (epithelium → lamina propria → muscularis mucosa)
submucosa
muscularis propria

Label the following diagram?


What are the three layers of the stomach?
- gastric mucosa and columnar epithelium
- non-specialised (antrum) or specialised (body) glands in lamina propria
- mucalaris mucosae
Where are goblet cells usually found and what do goblet cells in the stomach indicate?
Intestine
intestinal metaplasia
which part of the somach contains the most specialised glands
body and fundus create acid and enzymes
where is H pylori associated gastritis often found?
antrum (and pyloric canal)
In a normal duodenum, what is the villous:crypt ratio, what type of cells are found?
2:1
glandular epithelium with goblet cells - intestinal type epithelium

What are the histological features of acute oesophagitis?
LOTS of neutrophils (acute inflammation)

What is the most common cause of acute oesophagitis?
GORD
What are the most common complications to remember of most GI pathologies?
Ulceration
Haemorrhage
Perforation
Stricture
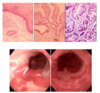
Recall the aetiology of Barret’s oesophagus
metaplastic process (squamous → columnar epithelium) in lower oesophagus
AKA columnar-lined oesophagus (CLO)
What are the two types of Barret’s oesophagus?
CLO
metaplasia WITHOUT goblet cells
= gastric metaplasia
CLO with IM
metaplasia WITH goblet cells
= intestinal metaplasia (IM) - higher cancer risk
What is gastric metaplasia?
Metaplastic change in oesophagus without goblet cells
What is gastric intestinal type metaplasia?
Replacement of squamous epithelium with metaplastic columnar epithelium WITH goblet cells present
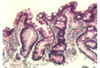
Describe the histological changes seen
- Normal
- CLO
- CLO with IM - contains goblet cells
If reflux oesophagitis causes a perforation of the oesophagus, what will be the result?
Mediastinitis
What is the most common sequence of pathological progression to cancer in the upper GIT?
Metaplasia –> dysplasia –> Cancer (flat pathway)
- Metaplasia (reversible)
- Dysplasia (some cytological/histological features of malignancy, no BM invasion)
- Adenocarcinoma - abnormal cells invade through BM
(as opp to lower GI - adenoma -> carcinoma pathway polyp)
What is the most common type of oesophageal carcinoma in developed coutries?
Adenocarcinoma
Where does adenocarcinoma of the oesophagus usually develop?
Lower oesophagus (bottom third)
Why is prognosis for oesophageal cancer particularly poor?
Most patients are not suitable for resection surgery
Which type of oesophageal cancer is most strongly associated with GORD?
Adenocarcinoma
What are some histological features of oesophageal adenocarcinoma?
Glandular epithelium
Mucin
What is the most common type of oesophageal cancer in developing coutries?
Squamous cell carcinoma


