Glycolysis Flashcards
(200 cards)
To lose one pound of weight, ones caloric intake should decrease by approximately how many calories?
1500
2000
2500
3000
3500
3500
In order to maintain his/her current weight, hw many calories will a 70 kg sedentary individual require daily?
1550
1850
2150
2450
2750
2150
(70 x 24 x 1.3 = 2150)
Under fasting conditions, which of the following is true?
Muscle glycolysis is inhibited
Liver glycolysis is inhibited
Muscle glycogen degradation is inhibited (it can be turned on
Liver glycogen degradation is inhibited
Liver glycolysis is inhibited (Muscle glycolysis won’t be inhibited under fasting conditions)
Still under initial fasting conditions which statement is correct (initial fasting conditions)?
Muscle glycogen synthesis increases
Adipocyte fate content increases
Urea synthesis increases
Lactate utilization by RBC increases
Urea synthesis increases (AA are now used as energy source and their waste is in urea)
What is diabetes?
Type 1?
Type 2?

What are you looking for?


A type 1 diabetic has just eaten, but forgot to take insulin. Which of the following will occur as a result?
Fatty acid degradation in the liver will increase
Glycogen degradation in the liver will decrease
Gluconeogenesis in the liver will continue
RBC’s will increase their oxidation of fatty acids
Gluconeogenesis in the liver will continue (In absence of insulin gluconeogenesis will continue. But glucose levels will actually continue to rise because insulin is required for glucose uptake by the muscle and the adipose tissue and liver still pumps out glucose via gluconeogenesis. Insulin is required to stimulate glycogen synthesis.)
(RBC’s have no mitochondria and therefore cannot oxidize FA)
(RBC’s have no mitochondria and therefore cannot oxidize FA)
Overview of Glycolysis
Two pathways of Glycolysis — Anaerobic and Aerobic
In order to generate Triglyceride we need to go through glycolysis.
Excess glucose goes through glycogen biosynthesis.

Glycolysis in Muscle vs. Liver

What type of metabolism is used when sprinting
Sprinting — Anaerobic Metabolism
Glucokinase is found…
Glucokinase — liver and pancreas.
Hexokinase is found…
In every other tissue but the liver and the pancreas
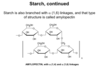
Glucose-1-Phosphate is Isomerized into…
Glucose 1 phosphate is isomerated into Glucose-6-P
What is the first committed step in glycolysis?
Phosphofructokinase 1 (PFK1) — Irreversible. Committed Step. Regulated Step.
How many ATP’s are used to get to the point of having two triose’s?
2 ATP
How does NAD become NADH?
Is this oxidization or reduction?
NAD+ accepts two electrons and a proton to become NADH
What is a mutase?
Whenever we move a phosphate from one functional group to another.
What is the function of dehydration?
Dehydration creates very high energy bond — about twice the energy of a high energy bond in ATP — ATP is 7kcal/mol where as the enolated phosphate is about 14 kcal/mol (which is doubled).
Which enzyme regenerates NAD so it can be reused?
Lactate Dehydrogenase regenerates NAD by converting NADH so it can be reused.
The Hexokinase Reaction

The Phosphohexose Isomerase Step

The Phosphofructokinase-1 Reaction (PFK-1)

Difference between Bisphosphate vs. Diphosphate

The Aldolase Reaciton